Solve Crossword Puzzles, Fund Abortions Across the Country
If you’ve been solving along with the Autostraddle mini and midi crossword puzzles over the last six months, you may have become familiar with the experience of seeing yourself and the things you care about represented in a puzzle. We (Rachel Fabi and Brooke Husic) are two of the crossword constructors for Autostraddle, and we have made it our mission to create puzzles that reflect queer joy and highlight some of the things we care about, and that we believe the solvers on Autostraddle also care about. To that end, we thought you might also be interested to know about a different passion project we’ve been working on for the past two years: a crossword puzzle fundraiser called These Puzzles Fund Abortion.
As anti-abortion laws spread around the country, we, along with our friend Claire, found ourselves grasping for a way to help people in need of abortion care. We brought together some of the best crossword constructors out there to create a pack of puzzles all themed around reproductive justice in order to raise money for abortion funds as part of an annual fundraiser hosted by the National Network of Abortion Funds (NNAF).
In exchange for donations that support five abortion funds around the country (the Baltimore Abortion Fund, Chicago Abortion Fund, Indigenous Women Rising, Tampa Bay Abortion Fund, and Wild West Access Fund of Nevada), you can receive a pack of 16 crossword puzzles that are all around the same level of difficulty as the A+ midi puzzles, or a New York Times Tuesday. Every dollar we raise goes straight to the funds we’re supporting, who in turn help people afford abortions, including support for their travel. We poured our hearts into this project, and we hope Autostraddle crossword lovers will join us in supporting abortion access through puzzles.
You can donate to receive the puzzles through our Fund-a-Thon page until May 31, 2023, after which the puzzles will be available through the These Puzzles Fund Abortion website. We are also selling TPFA merch through Bonfire until May 24.
Here’s a puzzle from the pack that you can solve today!
How Polyamory Pushed Me to Prioritize My Pelvic Health
I got my first yeast infection at 30. It was diagnosed during a pelvic exam with my primary care physician in December 2020, a month after my divorce was finalized. It was an especially painful exam because of the infection, and I wept for a long time when I got home. My ex and I were packing up to move to different states, but they took the time to talk me through some of my more complicated feelings: Namely, that I felt ashamed for “not taking care of myself” and thus getting an infection.
At the time, I felt ashamed about anything pertaining to my pelvic health. My first relationship had been an abusive nightmare in which my weight had been a point of contention — because if I were “less fat, then we could have better sex” — and that had a lasting impact on me. Then the partner I eventually married said I was hypersexual and would often ask me if I had showered recently when they could smell odor from my vagina — even if we were kissing or if they were touching me in a way that turned me on. I didn’t trust my libido or my body for a decade.
In July 2022, seven months into being one-third of a closed polycule, I was diagnosed with bacterial vaginosis and a severe UTI. This time I didn’t feel ashamed — I felt surprised. My symptoms were so sudden and so severe that I was forced to crawl out of the bathroom because the pain made me so weak. Both of my partners went with me to the emergency room, and we all thought this would be a one-time occurrence.
It wasn’t. That month alone, we went to the ER four or five times, and then I was admitted for a ten-day hospital stay. One doctor’s comment that I was “a bag of mysteries” became something of a motto each time I met a new provider. That was just the beginning. Fortunately, communicating openly and often about sex and pelvic health with my partners has helped me advocate for my needs, and now I’m finally on a path towards healing.
Deciding to explore polyamory for the first time at the start of 2022 was incredibly scary. In past relationships, polyamory had only ever been presented to me as a punishment or an ultimatum. Choosing to try it for myself felt empowering, but it also felt like skydiving with no parachute. I feared losing one or both of my partners, worried that I wouldn’t be able to handle my own feelings of jealousy, stressed about getting it wrong at every turn.
Sometimes I do get it wrong. All of us do. But by developing a strong base of communication and intentionally talking through issues as they arise instead of letting them fester, all three of us have been able to not only show up for ourselves, but also show up for each other. We set boundaries with each other and call each other in if those boundaries are violated. Our apologies include four parts: asking for consent, apologizing, naming what we’re apologizing for, and creating a plan for growth and improvement. We check in each day, often multiple times a day, to ask how we’re doing with our mental, emotional, and physical health; what tasks we need help accomplishing; and how we can support each other. We prioritize safety over productivity, and we strive to take each other at our word.
These practices translate directly to how we communicate about sex and intimacy. As a fat, chronically ill, increasingly disabled survivor whose sex drive created problems in my marriage, I’ve struggled to state what I want from my partners. I’ve feared that I want too much, too often, that seeking pleasure makes me selfish, and that asking to be touched in certain ways is too demanding. I’ve also worried that not wanting to have sex when my partners do will make them not want to sleep with me ever again. I’ve feared that saying “no” will birth bigger problems for us. In the last year, I’ve learned that none of these things are true and that being honest about what intimacy looks like for me at any given moment is the healthiest thing I can do.
By beginning to heal my relationship with intimacy, I’ve also begun to heal my relationship with my body. This has been especially integral due to how my body is changing. When I first started dating one of my partners, I began experiencing a new type of chronic pain that required me to walk with a cane. Suddenly, I had gone from having an invisible illness to being visibly disabled, which was difficult to process. I felt betrayed by my body and fearful of the future, especially as the pain got worse.
I’m a fat liberationist and genuinely love my fat body, and being with two other fat people has further radicalized me. But having sex as a chronically ill and disabled person is new to me. It requires me to be completely in my body during sex — something I avoided in past relationships to escape potential shame, pain, and discomfort. Now, for the first time, I have partners who encourage me to explore toys, tools, and positions that are as accessible as they are pleasurable. One of my partners also experiences chronic pain, and all three of us believe sex should be as shame-free and pleasurable as possible for everyone, however they choose to participate. For me, the way I participate in sex fluctuates constantly — especially because sex of any kind can be wildly painful.
Since my hospital stay last summer, I’ve exhausted the available urological tests and still struggle with persistent, resistant UTIs. I’ve been diagnosed with PCOS and may also have endometriosis. In December, I had a dilation and curettage procedure to determine whether my rapidly-thickening endometrial lining was cancerous. Thankfully, it wasn’t.
After a lifetime of being disregarded by doctors because I’m fat, I was accustomed to never getting answers — now, thanks to the communication skills I’ve practiced in my polycule, I refuse to be ignored. Instead of simply living with inconsistent and debilitating periods, chronic pain, and bizarre bladder symptoms because I’m afraid to acknowledge that something might be wrong, I’m advocating for myself. I ask my doctors to follow their hunches, encourage them to examine my symptoms from new angles, and ask scary questions. I demand to have tests and procedures done for peace of mind, even if they won’t reveal any new information. I state my boundaries upon meeting each and every doctor. If my boundaries as a patient are violated, I state that in the moment and then pursue new care paths with other providers. My ability to do this is a direct result of the communication and trust I’ve built with my partners in talking about sex, intimacy, illness, and pain. It also helps that I always have one, if not both, of them with me — and whenever I falter, I can silently communicate with them to step in and help me advocate for my needs.
The first time I considered asking for a hysterectomy was right before I got married. When I brought it up with my doctor, he told me it was an invasive procedure that required more thought than he believed I’d given it. Now, six years later, an OBGYN will be removing my uterus because I believe it’s the best thing for me, and she believes the procedure will grant me some of the freedom and relief I’m desperately seeking. Thanks to my self-advocacy and a bit of luck, I finally found a doctor who listens to and respects my needs in this arena and doesn’t pin my illnesses on my weight.
Were it not for my partners and our commitment to talking through everything, all the time, especially when we’re struggling, I think I’d still be suffering. Although I never could have predicted it, learning how to practice healthy polyamory has taught me how to advocate for my health needs without even a modicum of shame.
My Hysterectomy and Early Menopause Reshaped My Sexuality — So My Queerness Found New Spaces to Inhabit
There is a distinct smell to the place; handsome and even topiary, as if cultivated specifically for watering holes on the brink of implosion via neglect. The smell only congregates in relatively ancient places and spaces; to grok when you smell it, you must have a sort of affinity for old things. To me, the stench of mousy, mossy mold is intimately — and infinitely — charming. The smell has always smelled like freedom to me, because it is so undeniably impenitent.
It is karaoke night at Sullivan’s, a bar that used to be “dangerous.” It was better then, obviously. Now it is fraternal; the original, delightful decay and decadence of age and realness are now covered — or rather, smothered — by AXE body spray. The space — once smelly and old — repurposed into a shrine for khakis and boat shoes.
The renovations do not stop the woman I’m dating from grabbing the mic and mashing up Carly Rae Jepsen and Trent Reznor.
Head like a hole.
Call me maybe?
I fall in love with her immediately.
Back at my apartment, we watch lesbian porn and fuck each other into the morning.
But an additional ribbon of time unfurrows from our embraces, and I suddenly find that my body is buckled over in the kind of agony that seems to swing the self into the sweet hereafter, ever so slightly. My only comparison is giving birth; I see my child in my mind’s eye and wonder if I am actually going to die in this timeline, leaving her motherless.
I am conscious enough to know that something profound has happened but not conscious enough to imagine egress from it.
As it turns out, an exploding ovary is about as painful as giving birth, at least in my experience. This bodily oxidation is often punctuated by other culprits, as it was in my case. That is, a disease of the uterus, a disease that is often allowed to fester inside the bodies of those of us deemed incapable of narrative, those of us deemed “dramatic.”
I undergo an emergency hysterectomy because the endometriosis inside of me has matured and grown its own blood vessels. It hugs my uterus to other organs and reaches its damn-near-conscious tentacles into the hollows of my anus. Before going under for surgery, I remember all of the times, all of the years, I’d complained about pain, never to be believed.
And so here we are.
Stage Four Endometriosis.
I didn’t even know the disease had progressive stages.
Before I blackout entirely, I think, All I want in this wretched world is a fucking cheeseburger.
Had I died in surgery, this would have been my last thought in this plane of existence, and somehow, I believe this speaks volumes about who I am, fundamentally, as a human.
A year after my full hysterectomy — and subsequent menopause at the age of 32 — I am desperately waiting to hear from friends at Mandalay Bay in Las Vegas. A white man — as is often the case — has just won the record for deadliest mass shooting in the history of the United States, an appealing title, it would seem, for those in society given the most and yet somehow, producing the least.
My now ex-girlfriend spots me in distress outside of a local coffee shop. Reflecting her perennial generosity of spirit, she offers me comfort and then says, delicately, that she’s leaving town with her new girlfriend. Not only is she leaving town, she’s relocating to San Francisco, a city I will forever associate with making gay porn and creating queer communities with other sex workers.
The inertia of the moment feels like time travel. Hadn’t we just been in one another’s beds? She was my last lover, after all, and now she’s with someone new?
I espy my body as if from the outside and realize that it is almost 100 pounds heavier than when she and I were last entangled. Multiple timelines of violence and growth, expansion and extinction collapse in on each other and I have the distinct feeling that I’ve been left with nothing.
Empty. Dark. Cavernous. Large.
Good luck, is all I can muster. And I walk away.
I used to get turned on in libraries, before my hysterectomy.
Not because I had a specific lover in mind, necessarily, but because all of the wisdom therein appeared, to me, to be accrued in one singularity, a black hole of infinite potential.
It didn’t matter much the library; I got lovers’ butterflies inside new ones with Aerogel insulation and wildly colored acrylic railings just as I did in old ones with rolling oak ladders and neo-Greco atriums soaring over marble floors.
My lust-filled obsessions were indicative of my fetish for knowledge and, of course, my affinity for old things.
I was aroused by thoughts of growing; little did I know that once I reached my true size, I’d stop feeling aroused all together.
My birthday is in five months. I will be 39.
I used to keep a detailed, numerical record of my lovers because I took pride in amassing many. In my late twenties, I stopped the habit, after tallying more than one hundred.
And yet, in the spaces between my last girlfriend and my 39th birthday, I can count the number of lovers I’ve had on one hand. There is phenomenological immensity to this fact, and mostly because the quantitative change to my sluttiness has happened so swiftly. Indeed, I now identify as asexual.
Even if you count the men I fuck for money, my laundry list of lovers is still modest enough to appeal humble to the most priggish Puritan.
So here I am.
Single. Round. And pushing middle-age.
But I am also, now, preternaturally unapologetic and percussively boisterous. Where once I found solace in the sleepy mornings of post-coital vulnerability and sexually charged reciprocities, I am now content to spend my moments of existence companionless. Antithetical, perhaps, to the popular contention that having more sex will fix the plague of loneliness, my asexual queerness feels larger — unadulterated from social expectation and divorced from whoever may be in my bed at any particular moment. In this way, my queerness fills up the spaces I thought were reserved for other things: friendships, teaching, mothering, just to name a few.
That is to say, my dynamics with others are necessarily intimate, now, but not sexual. My queerness is too wild to be categorized. It has neither “management procedures,” as Foucault critiqued in his Repressive Hypothesis, nor is it situated within the “nature of public potential.”
Where once my sexuality flourished in the spaces of the unknown, it is now content to be still.
My structure of self, now a handsome and topiary smell to the empty, dark, cavernous, and large spaces of narrative, seems to be expanding into the vastness of space and time. I am alone. But I am large enough to let in the prism of light, reflecting back all the colors of the rainbow.
As a Nonbinary Abortion Activist, Planning a Pregnancy Is Complicated — And Hopeful
The day I get my IUD removed in the summer of 2022, my doctor asks me if I’m excited to have another baby.
I’ve just gotten off a consulting call with a new client, a reproductive health organization offering abortion services. A week prior, I helped crowdfund $5,000 for abortion funds, helped another organization write gender-inclusive language practices for their communications team, and sent a baby shower present to a friend expecting her second baby.
“Well,” I say. “It’s complicated.”
My compromise was to hire a doula who advertised as gender-, size-, and health-inclusive. She was the only person on my care team who took care to clarify my pronouns, to ask how I felt about gendered terms for my body and my parenting journey, to ask about my relationship and my identity and my values. During my 38-hour labor, she was the person who asked me if I consented to interventions, if I wanted to pause and take time to think, if I was ready to continue.
Months after I gave birth, after an unplanned C-section and a postpartum depression diagnosis and a relapse of PTSD, I wondered how that experience might have been different if I’d felt like I could be open about who I am. If there hadn’t been a part of me that was distracted by keeping the glass door on that closet, would I have been able to take more time? To ask for more space? To be less afraid to push back?
Even in the best of moments, pregnancy is an exercise in the unknown.
What if?
He moves for the first time when I’m in the middle of talking to a caller about her abortion experience two years prior. She and I are the same number of weeks pregnant. Her voice is uncertain, caught between anxiety and hope. She wants this time to be different.
When I tell a friend about it later, she asks me how it felt.
“Tender,” I say. “Honored. It takes a lot to trust someone with that kind of vulnerability.”
“No,” she says. “I meant about the baby.”
Is it unethical to have a baby when the world is literally on fire?
Will the people I organize with think less of me for having a baby right now?
How much of wanting another baby is about wanting to heal the trauma from my first pregnancy? If the answer is “any,” is that too selfish?
I read even more femme now than I did with my last pregnancy — is it even worth it to try to be out to doctors?
Is trying to get pregnant right now hopeful or insane?
Her answer:
“Does it matter?”
During my pregnancy, I start and stop half a dozen books, unable to get through the gender essentialism. Your body was made for this, mama. Women have been doing this for generations. This is the core of divine femininity.
In The Natural Mother of the Child: A Memoir of Nonbinary Parenthood, Krys Malcolm Belc Writes, “Nothing about being pregnant made me feel feminine. This body is what it is: not quite man, not quite woman, but with the parts to create and shape life.”
Yes.
I take notes on direct action and legislative advocacy and clinic support in a FUCK ABORTION BANS T-shirt with a bottle of prenatal vitamins sitting on the corner of my desk. On the other side of my office door, I can hear my toddler sprinting through the house, followed by two attentive dogs and one attentive parent.
It is the calmest I’ve felt in weeks.
“Well,” I say. “It’s kind of a weird time to have a baby.”
“Oh, honey,” she says, picking up her forceps to remove my IUD. “Isn’t it always?”
I’m Sick of White Women Centering Themselves in the Struggle For Reproductive Justice
Feature image via Georgia State University Library Exhibits.
This piece has been a long time coming. On June 24th, 2022, I sat next to my mother on the couch in our family home. Some trashy reality television was probably playing in the background. I checked my phone and I see the notification from CNN on my phone.
Like so many people, the devastation I feel about the Supreme Court’s federal ban on abortions is to a point where words don’t feel adequate. We all have the right to feel our pain and express our pain. No one should dismiss or invalidate anyone’s hurt. Sharing my pain about the ruling with others – talking freely and crying out frustrations with loved ones in safe spaces – is one of the most effective ways of coping for me, personally. Community is healing.
While trying to process everything, I noticed a certain pattern of comments from tapping through Instagram stories and popular Tik Tok videos on my FYP:
“I can’t believe women no longer have reproductive justice.”
“The position of women in society is going backward.”
“Women’s rights were taken away.”
All of these comments carry truth, and I’m not trying to completely negate them. The overturning of Roe v. Wade is a major step back. But, these comments are over-generalizations. We need to be intersectional and reframe our conversations surrounding reproductive justice. Womanhood isn’t an isolated identity and it isn’t a monolithic group. What white cis women today are experiencing is what women of color have experienced for decades, for centuries. Black women are routinely denied or mistreated in reproductive healthcare to the point where the lives of Black women are at risk. Modern gynecology exists because of cruel experiments that were forced upon enslaved women in America. There is a long and extensive history of the bodies of women of color being exploited in “the name of medical progress,” misunderstood, and not receiving necessary care.
Also, these comments erase trans, gender nonconforming, and nonbinary (TGNC) folks from the fight for reproductive justice. According to the Positive Women’s Network’s page on trans-centered reproductive justice, “One in three TGNC people delayed or avoided preventive health care, like a pelvic exam of STI screening, out of fear of discrimination or disrespect. This number is even higher – almost one in two — for transgender men.” Many trans people buy hormones outside of the health care system because they do not have adequate resources to safely obtain them.
There are even worse comments like:
“You messed with the wrong generation.”
“This time, we’re serious.”
These so-called “witty” social media captions are ignorant and disrespectful to history and activists who put immense physical and emotional labor toward freedom and liberation. Also, what does “we’re” mean exactly? Who’s “we”? It seems like the people behind these comments are trying to speak for everyone and putting themselves at the center.
Time and time again, many white women only stand up when it directly affects them. As a cis Latina, I know I can’t speak for every group. I will say that I’m tired. I’m tired of the white women that come to protests in Handmaid’s Tale costumes and hold up signs that say “we are the granddaughters of the witches you couldn’t burn.” I’m tired of performative activism on social media. I’m tired of the conversations that exclude the distinct issues of women of color and TGNC people in reproductive justice.
Why has this piece been a long time coming? One reason I struggled to accept is that I was afraid of upsetting people. I was afraid of comments that went along the lines of “not everything has to be about race” (everything is about race) or “you’re blowing it out of proportion”. But, I’m not responsible for white fragility, nor should I coddle it. I don’t want my silence to contribute to the erasure of TGNC people.
Whiteness needs to be decentered from the fight for reproductive justice. I’ve always said that history is a powerful tool for transformation and rethinking – I want to share a piece of history that does just that, the history of mass sterilization and reproductive genocide of Puerto Rican women between the 1930s to 1970s.
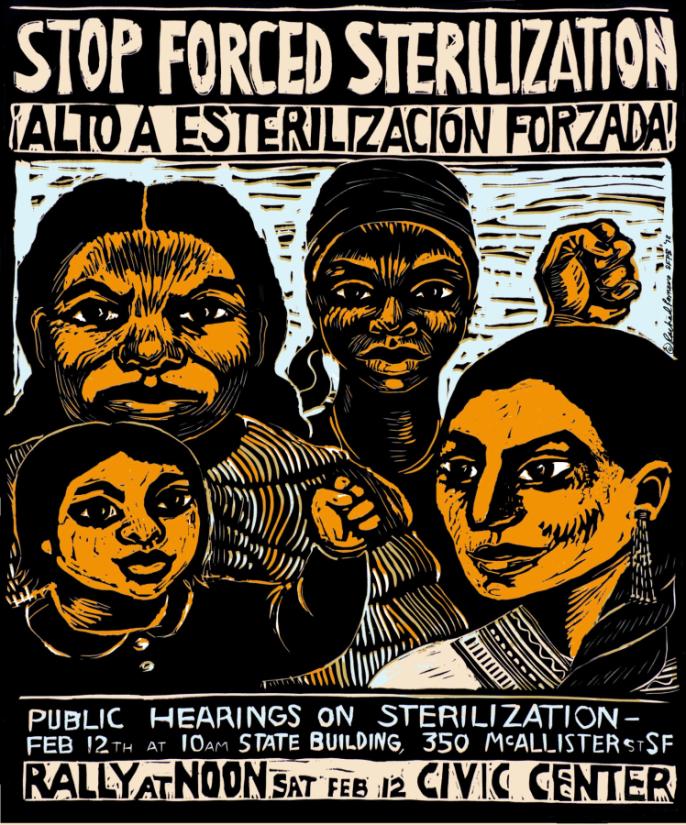
HHR, ““Stop Forced Sterilization,” c. Rachael Romero, San Francisco Poster Brigade, 1977,” Georgia State University Library Exhibits, accessed August 26, 2022.
I learned the history of reproductive genocide in Puerto Rico during my last year of high school. I was never taught it in a class – I searched for the information on my own from a yearning to learn more about who I was and my history. During my time in a former organization on my college campus called Planned Parenthood Generation, I worked with another member of the group (and the only other woman of color in it) to organize a panel that addressed the history of the struggle for reproductive justice for women of color. I made it my mission to bring up the sterilizations and cruel experiments performed on Puerto Rican women because silence is erasure. It is my mission now to use this history to expand dominant conversations on reproductive justice.
Freedom of any kind looks different for everybody, but my favorite definition of reproductive justice is from SisterSong Women of Color Reproductive Justice Collective, which states that Reproductive Justice is the:
“human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.”
The only thing I’d add to that definition is that reproductive issue is a human right regardless of race, gender, class, and ability. Reproductive justice is not just a woman’s issue. It is an issue of white supremacy, colonialism, capitalism, homophobia, ableism, and transphobia. It should always be at the forefront of human rights movements regardless of whether white cis women are directly affected or not.
A quick history lesson to understand the main history lesson. Puerto Rico was originally called Borikén and was inhabited largely by Tainos. In 1493, the Spanish invaded, colonized, and renamed the island. In 1917, The United States claimed colonizer status of Puerto Rico from the Spanish-American War. Puerto Rico’s been a colony ever since, and while it’s technically labeled as a “commonwealth” or “U.S. territory”, I don’t want to use any bullshit sugarcoating or euphemisms to hide the inherent violence of colonialism. This context is critical to understand because the U.S.’s reproductive control over Puerto Rican women’s bodies was a demonstration of colonial power.
The acquisition of Puerto Rico was a part of this fantasy U.S. rulers had of Manifest Destiny. American expansion was encouraged in the name of “civilizing” nonwhite individuals in different lands. So it was basically having a white savior and god complex. There was also an enthrallment with “neo-Malthusian theory,” a belief that “population control” was essential to human survival and connected economic status with genetics. The underlying logic behind it was that the rich were rich because of “good genes” and the poor were poor because of “bad genes.” Do y’all see this pattern of coded language? Anyway, the theory also dictated that it was the responsibility of the rich to dispose of the poor or else they’d be a detriment to society and cause overpopulation. These ideas fueled the rise of eugenics, which was at the root of the mass sterilization of Puerto Rican women.
Charles Herbert Allen, a U.S.-born politician, became the first governor of Puerto Rico after the U.S. seized the island. In his view, the island was “underdeveloped” because of overpopulation and the “excess” of people needed to be “taken care of.” Fuck centuries of colonialism and the denial of sovereignty as the roots of problems within Puerto Rico, I guess.

Puerto Rico, 1960. (Hank Walker/The LIFE Picture Collection via Getty Images)
Law 116, which allowed sterilization surgeries, was passed in Puerto Rico in 1937. Health workers visited many family homes and pushed mothers to undergo hysterectomies or tubal ligations. In 1953, 17% were sterilized. In 1975, 35% were sterilized and the average age at the time of the operation was 26 years old. These surgeries were so common that they were simply called La Operación or “The Operation.” Many of these women were uninformed that these surgeries meant they would become permanently infertile and were under the impression that the inability to reproduce was temporary.
Puerto Rico was used as a laboratory by U.S. eugenicist Clarence Gamble, who tested contraceptives that were not approved by the FDA on over a thousand Puerto Rican women. The popular birth control pill we know today was tested on Puerto Rican women with the encouragement and help of Gamble. The women were informed that the drugs given to them were used to prevent pregnancy, but had no idea that they were test subjects. There were women who were severely sick, and women that died. It didn’t matter if these experiments caused irreversible damage to their bodies – they were disposable in the eyes of eugenicists. It did not matter because upper-class white women, who were the first main consumers of the pill, were able to advance their mobility.
Eventually, the trials and experiments ended. But by the end of the 1970s, one-third of all Puerto Rican women were sterilized.
The denial of reproductive freedom and autonomy has been orchestrated beyond the overturning of Roe v. Wade. This is just one of the plethora of examples of a marginalized group being denied reproductive freedom and autonomy.
James Baldwin once said “History is not the past. It is the present. We carry our history with us. We are our history.” History also isn’t a series of isolated events. Everything is connected — Law 116 and the fall of Roe v. Wade are violent demonstrations of bodies being denied autonomy. They also involve, albeit in different ways, white people elevating themselves and their power.
The first step toward whiteness being decentered in the fight for reproductive justice and implementing intersectionality in praxis and discourse is to listen to different voices from different marginalized groups. Bring women of color to the front, burn the table that allows white supremacy to flourish, and work toward building a new, more inclusive table. It’s not going to solve everything. But it’s a start.
If you would like to learn more about the dark history of sterilization in Puerto Rico, below are a few sources I recommend and where I got my information from:
Matters of Choice: Puerto Rican Women’s Struggle for Reproductive Freedom by Iris Lopez
La Operación (1982) directed by Ana Maria Garcia
Reproducing Empire: Race, Sex, Science, and U.S. Imperialism in Puerto Rico by Laura Briggs
Needing To Abort Due To a Life-Limiting Fetal Diagnosis Was Heartbreaking Enough Already
Torre hadn’t always wanted to have kids — she was, after all, once a ‘90s punk rock teen who believed procreation was a self-serving planet-destroying impulse — but she began feeling the pull to parent in her 20s, and by her late 30s, her biological clock was ticking hard. Still, she didn’t feel financially or emotionally ready to parent alone. But then she met Oshin — they were a customer at the bougie pet store in Portland where Torre worked — fell in love, moved in together during the pandemic, realized they both wanted to be parents, and began the arduous process that is Trying to Conceive as a Queer Person. There were fertility drugs and a difficult and expensive search for a sperm donor who was, like Oshin, Armenian; and concerns that at the age of 40, it’d be difficult to conceive. But after four rounds of IUI, Torre and Oshin got the good news in December of 2021: They were pregnant!
“I was shocked and in disbelief but oh so happy,” Torre remembers. She was with her family in Denver when she got the news, and immediately told her Mom and sister. They decided to nickname the baby ‘Angelfish,’ an idea that’d come to Torre’s Mom in a dream she’d had about her daughter being pregnant a few years prior. By the time they made their pregnancy announcement on social media at 12 weeks, most of Torre’s close friends already knew.

Oshin and Torre with their first Ultrasound picture. Photograph by Kael Tarog
“The room felt like it was shrinking.”
Three days after making that announcement, Torre and Oshin were beaming, expectant parents at a doctor’s appointment. Their sonographer had just taken an ultrasound, and they were taking pictures of it and sending it to their friends along with recordings of their baby’s heartbeat when the doctor entered the room and began: “Unfortunately…”
“My heart started pounding, I could barely hear what she was saying,” Torre recalls. “Something about the nuchal translucency being the wrong measurement. The room felt like it was shrinking. I tried to keep breathing. Oshin gripped my hand.”
The doctor explained there was a good chance the baby had chromosomal issues, and they could wait it out or do additional testing. They opted for a blood test and a chorionic villus sampling (CVS) biopsy, a prenatal test that takes a tissue sample from the tissue that will become the placenta.
Trisomy 18, or Edwards Syndrome, occurs in around 1 out of every 2,500 pregnancies and is caused by an error that happens during sperm or egg formation. Abnormal chromosome segregation (division of DNA) during formation of sperm or egg leads to a sperm or egg with two copies of chromosome 18 instead of one, thus creating an embryo with three copies of that chromosome. It’s a random and unpredictable event that a parent can’t cause or control, but chromosomal abnormalities are more likely to occur in parents of advanced age.
95% of trisomy 18 fetuses don’t survive full term. Genetically abnormal pregnancies typically end in early miscarriage, and of those that are diagnosed later in pregnancy in utero — typically around 12 weeks — 85% will not survive and instead will lead to a later miscarriage, intrauterine demise, or a stillborn birth. Of those who make it to delivery, only 50% survive two weeks, and under 5-10% survive past their first year.
But living with trisomy 18 isn’t easy, as it causes severe abnormalities in nearly every organ system. Children born with trisomy 18 generally struggle to breathe or eat and typically present with severe heart, gastrointestinal, and neurological defects, as well as significant developmental delays.
Rarely, doctors may offer potentially life-extending treatments like cardiac surgery to trisomy 18 babies, but infants with trisomy 18 are less likely than other babies to survive these surgeries. Because of the degree of lethality, most doctors recommend no intensive intervention and only supportive comfort care for infants born with trisomy 18.
After consulting with their medical team, Torre and Oshin chose to terminate the pregnancy. “As gut wrenching as it was, we felt that the least suffering for our Angelfish, Oshin, and me would come from saying goodbye,” she remembers.
After waiting a week due to pandemic staffing shortages, Torre had a fully sedated dilation and evacuation (D&E) at 15 weeks. “I woke up feeling deeply changed, to my core,” Torre says. “This type of grief is so intangible and crazy-making.” She felt blessed to have such a supportive partner and community. Her doctor provided resources, she saw a counselor, and her mother flew out to help her in the immediate aftermath.

The mantle shrine to Angelfish. “I have no recollection of taking it, but it’s from my phone,” Torre says of the photo. “It was all such a dark blur.”
When Your Only Option Is No Option At All
Choosing to terminate a planned pregnancy due to a life-limiting fetal diagnosis isn’t easy, especially for queer families or others struggling with infertility who have put significant financial resources and time into the process. But following the overturning of Roe v. Wade, termination won’t be an option at all for many parents and may impact whether parents in those states even try to conceive at all.
While the conversation around abortion rights tends to focus on unwanted pregnancies and those that pose a threat to the mother’s physical health, life-limiting diagnoses are a less-discussed reason a parent may require abortion care — and may need to do so later in their pregnancy.
Even before the Supreme Court’s devastating decision in June of 2022, it was already difficult-to-impossible for many people to terminate pregnancies due to “incompatible with life” prognoses for the fetus — it’s expensive, rarely covered by insurance, and already required travel and jumping through multiple hoops for those living in areas with heavily restricted abortions. In some states, doctors are prohibited from informing their patients that termination is an option, leaving parents to simply wait for what will likely be a miscarriage or stillbirth, while others will do their own research and elect to travel out-of-state to receive an abortion.
“It’s traumatic enough to have to end your baby’s life,” writes Kelcey of her trisomy 18 baby on Shout Your Abortion. “I still felt guilt and shame for the choice that I made. Having to go out of state and stay in a strange place, having so little support and the stigma attached made it so much worse.”
“Carrying a pregnancy for weeks knowing it’s not viable and needs to be terminated is brutal.”
Confirming a life-limiting fetal diagnosis — defined as “lethal fetal conditions as well as others for which there is little to no prospect of long-term ex utero survival without severe morbidity or extremely poor quality of life, and for which there is no cure,” which includes a multitude of cardiac defects as well as trisomy 18 and trisomy 13 (Patau Syndrome) — can take time.
The first diagnostic tests are available at 10-13 weeks, and confirmatory tests and results can take a few more. The worst case scenario is one in which a parent lacks insurance coverage for genetic testing and can’t afford the out-of-pocket fee and therefore doesn’t get a diagnosis until their 20-week ultrasound — but any scenario will put many parents in a terrifying time crunch, depending on their home state’s specific restrictions. Abortion providers in states like New Mexico, on the border with Texas, are already seeing incredibly long wait times for appointments, if a parent is able to get an appointment at all.
“Abortions are safer the earlier they happen in a pregnancy,” Dr. Elizabeth Rubin, a board-certified OB/GYN in Oregon who was one of Torre’s doctors, explained to me. “So what they’re doing is taking someone who already has a heartbreaking diagnosis, already is going through hell, and slapping an extra dose of unsafe onto it — adding unnecessary time pressure, schedule/travel stress, shaming and morbidity to a safe procedure — and adding to their recovery time. And honestly, really f*cking with their mental health.”
Another hopeful mother on SYA shares a story where, despite living in California; due to limited options from her local Catholic-controlled healthcare system and a totally-booked Planned Parenthood, wasn’t able to terminate her trisomy 18 baby until just shy of 22 weeks, after a friend of a friend called in a favor to the dean of her local medical school. “Carrying a pregnancy for weeks knowing it’s not viable and needs to be terminated is brutal,” she writes. “In those weeks I had no choice, I didn’t have the healthcare I needed.”
If forced to endure an excessive wait time or unable to abort at all, parents will likely miscarry. “It sucks to get the option of a D+E under controlled circumstances taken away from you,” Dr. Rubin explained, “and instead you have a miscarriage at home in your bathroom and then have to go to the hospital and have a D+C for the placenta. Like, that sucks! And it doesn’t have to be that way! That can be predicted and avoided.”
“Patients deserve the chance to know their options.”
When such a condition is diagnosed, doctors are advised to engage in Perinatal Palliative Consultation, a care strategy that focuses on “ameliorating suffering and honoring patient values,” presenting options including either terminating the pregnancy or continuing with it and then developing a post-birth care plan where one must choose priorities such as life prolongation or comfort.
“One of the most important parts of medicine, especially in gynecology, is shared decision-making,” Dr. Rubin told me. “Patients deserve the chance to know their options and think them through — that’s actually part of the grieving process.”
“I’ve seen families who have said, I love my child and want to do everything I can to help her live,” doctor Thomas Collins told Stanford Medicine, “and other, similar families who love their kids just as much who have said ‘In our family that is not living; it’s torture.’”
“We could not protect our daughter from trisomy 18, but we could shield her from any pain or agony that would come with it,” wrote Allison Chang, a then-medical student at Harvard, in an essay about her trisomy 18 experience. Chang recalled her relatively humane, while still traumatizing, experience terminating her pregnancy in Massachusetts, compared to what her friend endured in Missouri, which included a hefty price tag and being “vaguely awake” during the procedure.
Different Choices for Different Parents
For “pro-life” parents, the path forward is clear-cut in a different direction. “We decided that if our son’s death was impending, we would not be the one to set that date,” writes the founder of Abel Speaks, a non-profit providing support for parents who’ve chosen to carry a child with a life-limiting diagnosis, in a video about the organization. “While losing Abel was tragic, the real tragedy would’ve been if we’d kept ourselves from truly loving Abel during the time when we did have him.”
Organizations and Instagram accounts like Abel Speaks emphasize that God has a plan for every life and that life doesn’t need to be long to have value. Their social media feeds solicit prayers for the passing of tiny humans who lived briefly and for pregnant couples (somehow exclusively photographed in grassy meadows) to have safe and smooth deliveries and a chance to meet their baby alive. They’re confident not only in God’s plan but in the existence of heaven and God’s readiness to accept and cherish their infant after its imminent passing. Many want the chance to Baptize their baby before the end of its life.
Abel Speaks is a window into a culture with very different values than my own and a religion very different from my own (I’m Jewish). Still, I can understand their perspective and appreciate their right to make decisions in accordance with their values. I’d even say that reading their stories did open my mind to another way of approaching a diagnosis like this, although it wouldn’t change the decision I’d make in their shoes, and I don’t think their religious or cultural beliefs should impact what choices are available to me or other parents with life-limiting fetal diagnosis.
That said, it’s not only religious and anti-choice parents who choose to keep a baby with a life-limiting diagnosis; some parents may choose to continue the pregnancy for other reasons, like that they feel they’ll have more closure being able to hold their baby than they would after a D&E. That, too, should be a choice, Dr. Rubin echoed: “Even for patients who decide they want to carry the pregnancy for as long as it lasts, or deliver, knowing that a doctor thinks an abortion is a reasonable alternative is important,” Dr. Rubin told me. “It also helps them to understand the gravity of the disease and their blamelessness, that this is not their fault.”
In this way, the life-limiting diagnosis debate illuminates precisely why choice is so important: Different parents have different values, priorities, and circumstances that lead them to make different decisions.
Pregnant people who don’t need to work may have more room in their lives for a pregnancy with such a difficult prognosis than those who need to be more pragmatic about their time off. People over 40 trying for their first child may know that termination is actually the option more likely to enable them to have a healthy baby, whereas a younger pregnant person might not feel that urgency. Parents who’ve already endured the trauma of a stillbirth may be more inclined to do what they can to prevent another.
The “best case scenario” for a child with trisomy 18 — living past that first year or longer, as famously has been true for Rick Santorum’s daughter Bella — is often still untenable for parents who, in a country starved of social services and health care, don’t have the time, financial resources, or health insurance to support a child who requires full-time care, or who already have children with special needs.
Instagram accounts like TFMR (terminating for medical reasons) Mamas offer support and visibility to parents who’ve had to terminate for a medical reason, who often feel ostracized from spaces for grieving a baby loss. This May, they held the first ever TFMR Awareness Day. Just over a month later, they were, posting in response to the Roe v. Wade overturning: “Having to navigate unnecessary barriers to the essential care that we need at this time creates so much extra distress on top of the unbearable heartbreak that TFMR parents are already trying to cope with… You don’t deserve this, our future TFMR parents don’t deserve this, I’m so sorry this is happening in 2022!”
“Since Roe v Wade was overturned I have been cycling through my own experience and just can’t fathom what it would have been like if, on top of our absolutely heart-crushing situation, I then had to worry about legalities and having to travel to have my procedure done,” Torre says. “I am really lucky to be living in a state where my right to an abortion is protected. Going back into trying again is already nerve-wracking, let alone having to worry about what I would do, or be allowed to do, if something goes wrong in future pregnancies.”
For patients pursuing fertility in states where abortion isn’t available, they will have to make a plan ahead of time for the possibility of a life-limiting diagnosis. This could mean paying out-of-pocket for a Cell-Free DNA screening earlier in pregnancy or even electing (the much more expensive option of) IVF rather than IUI because preimplantation genetic testing can examine the embryos prior to transfer for a range of genetic problems.
“These laws weren’t written by doctors, so they’re not written in ways that actually reflect medicine,” Dr. Rubin told me. “No one’s saying we could list the situations in which, say, a neurosurgeon could operate. Whomst amongst us could say we understand neurosurgery well enough to write legislation that determines when you can operate on a spine or a brain tumor? But because this involves pregnancy, they somehow think this should be something that everybody gets to weigh in on? And that lawmakers understand, even though they’re not doctors? There’s nothing I can think of in medicine quite like this.”
I’m Trans, I’m Trying to Get Pregnant and I’m More Pro-Choice Than Ever
I’m in what’s called the TWW — the two week waiting period between insemination and a missed period, or a period that comes and dashes all your hopes that the insemination worked. I’m texting with my friend about whether or not I have the strength to endure the disappointment of a negative pregnancy test next week, whether or not I can maintain hope through what may be many insemination attempts. Then she texts me, “Fuck.”
Roe v. Wade has been overturned, today, as I lie here praying that I’m pregnant. And I have never been more pro-choice than I am in this moment.
I was raised to protest abortion, to pray outside of abortion clinics, to look forward to and celebrate this day. My two BFFs in high school were related to a man who shot an abortion doctor for Jesus, which they thought was probably okay. Now I’m a leftist adult trans person who had no qualms about leaving ‘Merica behind to live with my soulmate in her country, Canada, which has federally socialized healthcare, including abortion care.
I have a history of sexual abuse and sexual trauma perpetuated by cis-het men. Sticking a syringe inside myself and injecting sperm is not something I enjoy. But I want a baby, and I’m doing it my own way — in an Airbnb with my wife by my side. There’s historical evidence of widespread abortion and contraception advocacy across the world, and the knowledge developed by people who were trying to avoid pregnancy is the very knowledge my partner and I are using to get pregnant: tracking ovulation, using cervical cups, etc. Undergoing this process has shown me just how absurd anti-abortion rhetoric truly is.
I have to confess that as a masculine person who has never had voluntary sex with cis men and who can’t get someone else pregnant, I hadn’t thought about abortion as much as I should have until recently. I have a uterus, which means I could be assaulted and could get pregnant against my will. Still, I thought, conversations about abortion didn’t really apply to me. I listened to the women I knew who’d had abortions (most of my partners, many of my friends and nearly every feminist thinker I’d learned from). When I lived in the US, I marched and voted and organized and signed up to drive people from rural areas to abortion clinics in Pittsburgh. And still, I didn’t think I would ever have to make a choice about having an abortion myself — until I decided to try and carry a child.
Before we started the fertility process, my wife and I had a conversation about whether or not, or when, we might have to make this choice. At 37, bearded and without tits, I finally weighed it out for myself. My wife and I agreed that we will probably opt for abortion in certain cases — for example, if the fetus has anencephaly. That’s when the skull and brain of the fetus do not grow and there is literally no hope that the baby will live beyond a few days after birth, if that, unconscious and in physical pain.
Since insemination, I’ve been nauseated every day, I’ve been disgusted by coffee (one of my favorite things) and salt (ditto), I’ve broken out with pimples in new places and I’ve been moody and emotional AF without my cannabis. Yet I walk around my neighborhood, I go to the store, I do all my normal activities — and no one else can tell. No one is passing me on the street saying, “Oh wow, there’s two of you now! There’s a person inside you!” Because even though I want to make a person with all of my heart, I am keenly aware that what’s happening inside me is a long and complicated process; there’s no magical instance when suddenly there’s an autonomous, separate human inside me.
The “pro-life” movement, codified by conservative Republicans, uses terms like “holocaust” and “genocide” to describe abortions, though they are politically aligned with literal holocaust deniers, rapists, child molesters, cops, border patrol agents and racists who participate in the continual genocide, oppression and sometimes even forced sterilization of marginalized people on this continent — especially BIPOC. The irony is intense.
I’m from a Catholic background similar to the culture that produced Amy Coney Barrett, although not as economically elite as the culture that produced Bret Kavanaugh. I can attest that the overturn of Roe v. Wade is a high holy day in their worlds. But while Catholics have been some of the key authors of anti-choice rhetoric, a 2014 study by the Guttmacher Institute found that Catholics have more abortions than Protestants, and Christians have more abortions than most other religiously-affiliated folks. Rich, white Christians and conservatives (and especially their mistresses) will continue to have safe abortion access in many instances, even if they have to cross state lines or fly out of the country to get one.
While Republican-appointed Supreme Court Justices are stripping people in the US of abortion rights, conservatives all over the world are coming for trans people, especially trans kids who have the courage to come out and ask for what they need. They’re making rules about when we can access the healthcare we need to survive, to grow up, to live our lives. While FINA has declared that swimmers must fully transition by twelve to be eligible to compete, parents in some states are being criminalized for allowing their children to get transgender health services if they are younger than eighteen.
When I moved to Canada and could get top surgery without a million consults or a letter from a psychiatrist — and at a fraction of the cost it would be in the US — I got a taste of what it feels like to have bodily autonomy. This sense of autonomy has enabled me to envision being pregnant. Without being able to assert my masculinity by coming out, letting my goatee grow and having top surgery, I would never have been able to imagine doing such a “feminine” thing as getting pregnant. According to the religious right, producing another human person is the most important thing I could ever do. Yet without actual bodily autonomy — including the right to have an abortion — I could never have started this process.
In the same way the Supreme Court is now saying that people with uteruses should be forced to carry fetuses to term, those who prevent trans kids and teens from accessing transition-related care are also forcing people to live in bodies that are not their own. When a country limits the individual’s autonomy over their own body, that is an assault on the people who live in that country — not just on the people with uteruses, but an assault on everyone.
Medication Abortion 101
Today is a heavy and unprecedented day. Whatever you are feeling today is valid and I hope you allow yourself space to take care of yourself this weekend. My “day job” is working as a campaigner at a gender justice advocacy organization where we have been prepping for this moment for months and preparing to fight back and identify opportunities to help those most impacted. In my “day job,” I focus on fighting online disinformation and misogyny online and I’ve learned that one of the best ways to fight false information is through sharing the truth.So I’m here to provide a small ray of hope and accurate medical information (though I am not a doctor, just a reproductive rights activist) about medication abortion.
Medication abortion is safe, effective and fully FDA approved and it can be accessed by mail, which means it will remain an option in states that now ban or even criminalize abortion, albeit with some risk attached in the states where it is criminalized. Here is everything I know about medication abortion so that you can access the care you need, share it with a friend, or save it for that just-in-case moment.
What Is Medication Abortion?
Medication abortion is a non-invasive combination of two medications, Mifepristone and Misoprostol, that work together to end an early pregnancy. It is FDA approved for the first 10 weeks of pregnancy but some providers will prescribe it off-label later in pregnancy.
It has a 95% success rate, and less than 0.5% of patients experience serious complications. Most abortions in the United States are already done through medication abortion and that number is likely to continue rising.
How Does Medication Abortion Work?
Mifepristone stops pregnancy growth by blocking the hormone progesterone. Progesterone helps the uterus grow in early pregnancy and keeps it from contracting so Mifepristone helps counter these effects. Misoprostol, taken at a later time, makes the uterus contract. Patients take Mifepristone to start the process followed by Misoprostol one or two days later.
Is This the Same as Plan B?
No, Plan B is over-the-counter emergency contraception that helps stop a pregnancy before it takes hold, medication abortion is a prescription regimen of multiple pills to stop an early pregnancy.
Is Medication Abortion Safe?
Yes, Mifepristone and Misoprostol have a long record of safe use. They have been approved by the FDA for more than 20 years and have been approved in France, Sweden, and the United Kingdom since at least the early 1990s. Mifepristone actually has a better safety record than penicillin, Viagra, and even Tylenol.
These medications are also regularly used to treat other medical conditions. Mifepristone can treat high blood sugar in people with Cushing’s Syndrome and Misoprostol helps prevent stomach ulcers.
What’s the Legal Situation Now?
In this new post-Roe world, things are unfortunately complicated but that’s not to say there aren’t options.
In 2021, the FDA removed the requirement for Misoprostol to be given in person in a medical setting and made it so that patients could access it via mail. Of course, that means in reaction, a bunch of laws were passed placing unnecessary restrictions and hoops in the way of accessing what should be a straightforward FDA-approved prescription. Today’s ruling complicated things even further; it means there are now many states with abortion bans and a few states where abortion is criminalized.
Thankfully, there are a few reliable websites (see below) that have done all of the research and have state-by-state information on how to access these pills within the legal confines of your state. In some places that may mean delving into legal grey areas, like using mail forwarding. I am not a lawyer and I’m not recommending you do something that will get you into legal trouble but as Mahatma Gandhi wrote in Non-violence in Peace and War “An unjust law is itself a species of violence.”
How Can I Access It?
There are a few websites you can try and see what has the best options for you in your state. I am a particular fan of Plan C because it lists resources and options available in places like Texas and Oklahoma, including things like getting a prescriber in the Netherlands and using mail forwarding.
What Should I Expect if I Take It?
According to Planned Parenthood the second medication, Misoprostol will likely cause fatigue for a few days, tender breasts if you have breasts, chills, fever, and nausea and you can expect to experience cramping and bleeding.
Can I Stock Up and Save It Just in Case?
In theory, these two medications are shelf-stable and could be acquired now and saved for a few years for a moment of need and it’s likely this will become a more popular, underground option. Again, I’m not a lawyer or a doctor so I can’t tell you how to make that decision. I can tell you that you will need a prescriber to get the medication in the first place and that Mifepristone has a shelf life of five years and Misoprostol has a shelf life of two years.
I Heard You Can Reverse It Is That True?
Abortion reversal refers to an experimental and dangerous procedure that has been promoted by anti-choice activists and physicians. They claim that by taking a large amount of progesterone — the hormones that Mifepristone blocks — and skipping the Misoprostol, it is possible to “reverse” an abortion.
There has only been one medical study ever attempted on this process and it was stopped early because it was deemed too unsafe to continue. Three people in the study were sent to the emergency room because of dangerous hemorrhaging. Both the American Medical Association and the American College of Obstetricians and Gynecologists have denounced medication abortion reversal.
89 Abortion Funds That You Can Give To Immediately
Feature image by Alex Wong/Getty Images.
Today, I am numb.
I haven’t been able to wrap my head around today’s Supreme Court ruling without a fresh wave of nausea. We all knew it was coming, right? We knew back in May when an early leaked draft of today’s decision first circulated. We knew in the years before that. We knew that the end game has always been Roe v. Wade.
It was always coming, and today was the day.
In today’s decision to the case Dobbs v. Jackson Women’s Health Organization — which is about a Mississippi law banning abortion at 15 weeks — in unambiguous language, and a 6-3 majority vote, the Court overturned Roe, as well as another case, Planned Parenthood v. Casey, which upheld the central tenet of Roe but allowed states to restrict access as long as they did not place “an undue burden” on people seeking abortions. From the decision, “We therefore hold that the Constitution does not confer a right to abortion. Roe and Casey must be overruled, and the authority to regulate abortion must be returned to the people and their elected representatives.” (You can read a full annotated version of the decision yourself.)
What comes next is overwhelming and can feel impossible. But what I do know is this — the fight is not done. It can’t be. 50 years ago we were promised a legal right our bodies and a group of extremists made it their life’s work to have that right taken back away. But if they can dedicate their lives to undoing the work of Roe, then I can surely dedicate mine to making sure those rights become enshrined, protected, and never taken away again.
I wanted to highlight at least one very specific, actionable thing you can do right now.
This post was originally written in 2021 and has been updated and republished twice this year, including today, because there is no way off this rollercoaster except to rely on ourselves, our advocacy, bear down and to fight.
What Is an Abortion Fund?
Over the last few months, you’ve probably seen calls to support abortion funds, and you’ll probably see more in the days and months to come. They provide financial and/or material (transportation, mental health care, volunteer assistance, etc) support to those who need an abortion. They’ve been around for decades. For those most vulnerable who need immediate aid now, and this is tangible way to show up and support.
You can donate (or learn how to volunteer!) with the organizations listed below.
As of today, right now, in about half of the states in the U.S., abortion has become severely restricted or outlawed. I have put an [*] next to states where abortions are restricted, likely to become prohibited, or where the future of abortion restrictions is uncertain in the days and weeks to come. I have put an an [**] next to states where, as of this writing, abortions are already banned. This comes from New York Times reporting, and as they update their states list, I will also update ours.
The purpose of this system is to draw attention to the inequity in safe abortion access in this country, and who is left with the least amount of resources available in light of today’s decision (and for many people, long before that, too). If you live in one of the 21 states, and DC, where the right to abortion is legally protected — recognize your privilege, and support beyond the guaranteed safety net your community.
Give to an Abortion Fund Today
Some of these funds have “women” in their title. Not all people who are in need of abortions are women. However, in the interest of providing the widest breadth of information to those who may be in need, in parts of the country where access is in immediate jeopardy, we only included funds that have “women” in the title if there was no other fund available in that state. We recognize it’s a delicate line, and one not one we take lightly. Safe abortion access is critical for trans patients, and should always be a priority.
Alaska
Alabama *
Arizona *
Abortion Fund of Arizona
Tucson Abortion Support Collective
Donate to Multiple Arizona Funds at Once, including Indigenous Women Rising (Arizona)
Arkansas *
California
Colorado
Cobalt Fund
Colorado Doula Project
Colorado Organization for Latina Opportunity and Reproductive Rights
District of Columbia
Delaware
Florida *
Florida Access Network
Emergency Medical Assistance Inc.
Tampa Bay Abortion Fund
ARC — Southeast
Donate to Multiple Florida Abortion Funds at Once
Georgia *
ARC — Southeast
The Feminist Center (Atlanta)
Hawaii
Idaho *
Illinois
Indiana *
Iowa *
Kansas *
Kentucky **
Louisiana **
Maine
Massachusetts
Abortion Rights Fund of Western Massachusetts
Eastern Massachusetts Abortion Fund
Jane Fund of Central Massachusetts
Maryland
Michigan *
Minnesota
HOTDISH Militia (Hand Over The Decision It’s Healthcare)
Our Justice’s Abortion Assistance Fund
Just the Pill
Mississippi *
Missouri **
Montana *
Nebraska *
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina *
North Dakota *
Ohio *
Oklahoma **
Oregon
Pennsylvania *
Rhode Island
South Carolina *
South Dakota **
Tennessee *
Texas *
The Afiya CenterThe Bridge Collective
The Clinic Access Support Network
Frontera Fund
Fund Texas Choice
Jane’s Due Process
Lilith Fund
Texas Equal Access Fund
West Fund
Utah **
Vermont
Virginia *
Blue Ridge Abortion Fund
DC Abortion Fund – VA
New River Abortion Access Fund
Richmond Reproductive Freedom Project
Hampton Roads Reproductive Justice League
Washington
West Virginia *
Wisconsin *
Wyoming *
We Will Protect Each Other: A Queer Feelings Atrium After the Fall of Roe
Ya’ll.
Maybe you knew it was coming. Maybe you were completely surprised. Regardless, no one wanted to tune in this morning to find that the Supreme Court of the United States had not just gutted but completely overturned Roe v. Wade. The court upheld the Mississippi abortion ban and overturned both Roe v. Wade and Planned Parenthood v. Casey. This turns the governance of abortion back to the states in the U.S.; in about half of the states in the U.S., abortion will become severely restricted or outlawed.
Fuck.
Shit.
I don’t have more eloquent words at the moment. Nor the time or brain power to go deeper on what this all means. Maybe you do. In the style of an old school feelings atrium, I’m here to talk today and to facilitate our community talking with each other. If you’re feeling a way – enraged, anxious, in mourning, nostalgic, fired up, like you need to scream into a void–this is a space to express that as well as anything else you need to get off your chest.
One thing I know for certain, we will protect each other. We’re here for each other.
So, how are you doing? What are you thinking? What do you need? I’ll meet you in the comments.
The Fall of Roe Is For All Of Us
Feature image art: Autostraddle, photo: Alex Wong/Getty Image
I was buying a vegan chickn wrap at a walk-up eatery near Syracuse University in 2006 when the cashier said, “I like your shirt!” The shirt was a black fitted tee with bright pink graphic lettering that read, “SAVE ROE!”
I was a professional campus organizer for a local affiliate of Planned Parenthood, and barely out of college myself. This was before the federal abortion ban and way before the current case before the Supreme Court and my work was primarily around expanding and protecting access to contraception.
Abortion bans and hostile restrictions were constantly on and off the table at the federal level, and there was a definite sense of anti-abortion extremists trying to chip away at the protections of the Roe v. Wade decision, but the idea that Roe would actually be overturned felt distant and vague and hyperbolic to a 23-year-old who had grown up in a post-Roe generation. I wore the shirt as a reminder to others of how important and how often fragile abortion rights were overall, not as a serious warning that Roe v. Wade might be gone in my lifetime.
Fast forward to Monday night, when I was checking slack for Met Gala hot takes after putting my five-year-old daughter, Remi, to bed and saw that my workplace chat was blowing up. Those of us closely following the Dobbs v. Jackson Women’s Health Organization (JWHO) case have known for months now that it’s extremely likely we’re on the precipice of the Supreme Court of the United States (SCOTUS) overturning Roe v. Wade. Abortion rights groups and repro justice groups and health providers and abortion funds have been planning and strategizing how to respond when that decision comes down later this year — likely in late June or early July. Working on everything from policy reform to creating community-based pathways to legal abortion when it becomes outlawed in almost half of the US.
Still, it felt like there was some bit of hope or at the very least, that it wasn’t yet a concrete reality yet, like maybe we could salvage something. In other words, the fact that SCOTUS was hearing this case meant they were open to reopening the decision on abortion, which was extremely alarming, but we were holding out hope that it was possible they wouldn’t fully outlaw abortion. We are still holding out hope — this isn’t over yet! But we need to move as if Roe is truly in peril, because it is.
On Monday night, a draft of Justice Samuel Alito’s majority opinion on the JWHO case was leaked to the press and it is… in a word… terrible. Terrible for abortion rights and access. Terrible for queer and trans people. Terrible for Black and brown people. Terrible for disabled people. Terrible for rural poor people. Terrible for Indigenous people. Terrible for immigrants without papers. Terrible. Terrible for all of us.
For the first time in my life, I’m absolutely certain that the conservative right is going to do everything they can to strip away the protections of the landmark Roe case. They’ve been trying to for decades, since Roe became the law of the land in 1973. That’s not new. But this is the first time I believe they may have the political power to do so, despite the fact that the majority of people in the U.S. regardless of which political party they belong to are supportive of legal abortion.
There’s a lot of confusion going around about what this all means and as someone who worked in repro and/or civil liberties work for over fifteen years, I’m here to demystify the moment we’re in right now. I’m not an attorney, but I used to play one on TV, so let me fill you in on what’s going on and what the potential end of Roe means for us.
Is abortion still legal?
Yes, abortion is still legal! Very much so. Despite some misleading headlines, SCOTUS has not voted on Dobbs v. JWHO yet.
The leaked opinion shows a clear intention for the currently presiding conservative majority to vote to overturn Roe, but it hasn’t actually happened yet. In fact, if you or anyone needs an abortion, you can find a provider at ineedanA.com or by texting “hello” to 202 883 4620.
Will abortion be legal if Roe is overturned?
Even if the JWHO vote happens and it results in a full repeal of federal abortion rights, some states will still have safe, legal abortion. Some states have trigger laws, state laws already on the books that ban or restrict abortion in the state. As long as Roe is standing, the federal protections for abortion mean that the state laws that conflict with Roe can’t be constitutionally enforced. If Roe is no longer the law and there is not sufficient federal law (which there currently isn’t), abortion bans or restrictions in those states will be able to go into effect and possibly be expanded. From the Guttmacher Institute:
“If Roe were overturned or fundamentally weakened, 22 states have laws or constitutional amendments already in place that would make them certain to attempt to ban abortion as quickly as possible. Anti-abortion policymakers in several of these states have also indicated that they will introduce legislation modeled after the Texas six-week abortion ban.
By the time the Supreme Court hears oral arguments in the Mississippi case, there will be nine states in this group with an abortion ban still on the books from before Roe v. Wade, 13 states with a trigger ban tied to Roe being overturned, five states with a near-total abortion ban enacted after Roe, 11 states with a six-week ban that is not in effect and one state (Texas) with a six-week ban that is in effect, one state with an eight-week ban that is not in effect and four states whose constitutions specifically bar a right to abortion. Some states have multiple types of bans in place.”
Why is this leaked opinion important?
The SCOTUS justices, while holding an appointed position and not an elected one, tend to correspond along Republican and Democratic lines, based on the party under which each justice is appointed. We tend to think of justices as either conservative, liberal, or moderate based on their voting records and backgrounds. Right now, three of the nine judges are decidedly conservative, and three are decidedly liberal. There are technically four moderates, but they were all appointed under a Republican administration.
There is and was some hope that the more moderate judges wouldn’t vote for a full repeal of Roe v. Wade, as there’s a possible outcome here that the vote is split on the question of a radical move like a full repeal. Instead, the decision could be made to more narrowly rule on the Mississippi law in question in the Dobbs v. JWHO case, likely voting to uphold the Mississippi law limiting abortion to fifteen weeks.
However, in the recent Texas case, which effectively eliminated abortion in Texas by criminalizing abortions after six weeks, Justice John Roberts voted with the liberal judges. Roberts is no pro-choice champion, to be clear and he has voted against abortion rights in the past. He represents a view that more strictly interprets the role of SCOTUS to not move quickly to divisive rulings or rulings that interfere with established precedent. He is also the chief justice, but other more moderate judges did not join him in taking a moderate approach on abortion in the recent Texas case, thus upholding Texas’ SB8 in a 5-4 vote. Two justices considered moderate (not in my opinion, but in general opinion), Kavanaugh and Barret, have both expressed an interest in overturning Roe, which means moving towards the middle to join Roberts seems unlikely.
So we come to a place of assuming Justice Alito, who is deeply conservative, is representing the majority opinion because we’ve been anticipating for quite a while that this court is hostile to abortion rights. The opinion itself is damning, not just for the end of Roe v. Wade, but the right to privacy established by several landmark SCOTUS cases including Roe v. Wade. It’s true that drafts of the majority and minority opinions are often worked on before the decision day, especially when it’s known or assumed what the outcome of the vote will be, so it’s possible this isn’t final. It has been confirmed as authentic, though, and it gives us a lot to worry about.
What are we worried about?
So many things. If we lose Roe, abortion will be banned in many states, making it much harder to access safe and legal abortions. People will need to travel thousands of miles depending on where they live. Many will be unable to afford that, and criminalizing abortion doesn’t mean abortions won’t happen. Abortion rates are not slowed when abortion is not legally available. Historically, we know that pregnant people will seek abortions regardless, but what should be an extremely safe and routine procedure becomes deadly when it’s criminalized. And those more impacted will be poor folks, Black and Latinx folks, young people, immigrants, and anyone without financial means to get on a plane and fly out to where abortions are still safe. Already, material mortality rates are significantly higher in states that have restrictions on abortion.
Beyond that, Roe v. Wade and reproductive rights, in general, are directly tied to establishing the constitutional right to privacy. That right is not enshrined in writing in the Constitution. It’s been established through legal precedents, like Griswold v. Connecticut, the case that first legalized birth control specifically for married couples in 1965, which established that there are “zones of privacy” inherent in the Constitution. Other repro cases like Eisenstadt v. Baird in 1972 and Roe v. Wade in 1973 expanded on this idea of privacy from government intrusion, eventually extending that right to the individual. In the case of Roe, it created a specific link between the due process clause of the Constitution and the right to privacy.
The landmark LGBTQ case, Lawrence v. Texas, which overturned homophobic anti-sodomy laws in 2003, directly quoted Roe and other repro cases to make the argument that the government should not interfere in consensual, adult sexual behavior in the home. Privacy rights again came into play in Obergefell v. Hodges, the 2015 SCOTUS ruling that legalized marriage across the US. We should be worried about this and more. Forced sterilization laws, interracial marriage, access to contraception, rights of sexual assault survivors, rights of sex workers, are all things on the table if Roe is overturned.
That said, the jumping from what is happening now to, “They’re coming for gay marriage next!” is not rooted in a real threat, today, right now, and also inherently implies that the current issue before SCOTUS is not an LGBTQ issue. It absolutely is.
Why does this matter for queer and trans people, in particular?
Queer and trans people have abortions, for any number of reasons. We and our partners have abortions and are too often facing double stigma, stigma and shame around receiving abortion care and stigma (unfortunately often by service providers) for being trans and/or queer. Abortion is not a “women’s issue” and it’s not a cisgender heterosexual issue. It’s our issue and it affects our communities and it’s deeply under threat. We have to act, not just because we are afraid of losing other rights in the future, but because this is about us and our people, right now. If our feminism is intersectional and if our belief is that our community matters, we need to see abortion as a queer issue and trans issue right now.
Ultimately, controlling reproductive choice is about controlling people’s bodies. Controlling “unruly” or “unfit” bodies is about upholding white supremacist patriarchy and capitalism. The right has an interest in promoting “traditional family values” as a way to enforce a capitalist system of labor. In other words, capitalism and white supremacy and patriarchy benefit from keeping men at work producing profit for owners and women at home producing children (a.k.a. more workers and wives). Demanding control of anyone whose body doesn’t fit into that narrow narrative or who doesn’t produce the desired value for the economy, whether that is Black and Indigenous people’s bodies, disabled bodies, queer and trans bodies, is not just sexist, racist, and ableist. It’s heteronormative and cisnormative. And all of it bottom-line holds up a capitalist system that only works if we subjugate pregnant people and anyone whose body is not participating in the “correct way” of producing for those in systemic power.
This isn’t theoretical jargon, it’s real. Trans bodies are under attack in state legislatures all over the country right now, powered by the same party and the same extremists that would delight in seeing abortion criminalized. During the long fight for marriage, time and again the main argument against it was that gay couples would be unfit parents (false) or that we could not biologically reproduce (also false) which was declared the basis of a good “traditional” marriage. The forced sterilization of Black women and Indigenous women and disabled women, a eugenics-rooted history that is far too recent and frequent, is absolutely about white people in power deciding whose bodies are best for reproduction to uphold white supremacy (which is, deeply, inherently ableist). We have shared enemies not because all so-called progressive issues are linked, but because we literally have the same enemies. And they are actively trying to control our bodies in a relentless aim to eradicate any deviation from a white supremacist cishet patriarchal society fueled by capitalism. Whew.
All that to say, this matters, not because we might lose marriage in the future, though I do also believe that’s a valid concern, but because this is about us, right damn now, and our people and loved ones. Our bodies are already under attack. Our people are already being harmed.
Abortion access and abortion rights are already a trans rights issue and a queer rights issue. We need to fight like hell, not “for them,” but “for us.”
Is there any way to stop this?
Kind of. There are possible remedies and, frankly, we have to pursue all of them ferociously. One option is that we pressure the Senate to pass the Women’s Health Protection Act, which would create an affirmative federal law codifying abortion rights. However, the Senate doesn’t have the necessary sixty votes to pass this bill, which has already passed the House of Representatives. And to change that, we would need to change the filibuster rules. That’s a real possibility, but we need to move fast and pressure our Senators to make it a reality quickly.
There is the possibility, always, of organizing and making our voices so loud that we can’t be ignored. It’s already true that the majority of Americans don’t want to see Roe v. Wade overturned. We need to show that power with our voices and our bodies. Already, there has been an enormous amount of public support for Roe and outrage about the leaked Alito opinion. Just hours after it was leaked, people were gathered in Washington, D.C. outside of the Supreme Court, and the steps of the court were packed all day on Tuesday. Around the US, marches and rallies are being organized as people everywhere go into the street to demand our rights. People power is one way we show, visibly and emphatically, that the vocal majority don’t agree with Justice Alito and the conservative court and that this is not the time to undo historic precedent by overturning Roe. The SCOTUS vote hasn’t happened yet and this is our opening to keep the pressure on those in power.
What can I do?
So many things!
- Donate to abortion funds — abortion funds help people pay for fees, transportation, hotel, and other personal expenses in order to access abortion.
- Ensure people know that abortion is still legal. Share and access INeedAnA.com, a resource to find vetted, up to date, and personalized info on how to get an abortion. You can also or text ‘hello’ to 202 883 4620 to get info.
- Join or organize national Bans Off Our Body actions across the country on May 14th.
- Share abortion stories. Share abortion access info. Share calls to action. Educate others! The Liberate Abortion Campaign has some great free graphics for social sharing.
- Wherever you are, contact your local abortion rights orgs to find out more about how to get involved.
- Do community care where you can. Check in with your loved ones and friends. Ask for what you need and give what you have as we collectively cycle through grief, anger, or any other very appropriate emotion.
This fight is far from over. Let’s take care of ourselves and each other, and know we will move forward from here taking care of our own, no matter what.
Have more info or resources to share or more questions to ask? Post them in the comments.
Anti-Blackness and Bioessentialism Won’t Give Us Abortion Rights
On September 1st, Texas passed the strictest abortion law in recent history.
“This is a terrible thing for women,” wrote my classmates in our group chat.
I texted back: “This is a terrible thing for anyone that can get pregnant.” The typical awkward silence happened before everyone moved on.
The next day, the world’s favorite Black gay troll Lil Nas X announced that he was “expecting” a little bundle of joy called MONTERO, his debut album. Two events, seemingly unrelated but ultimately tied together by what they reveal about our culture.
If nothing else, these two things reminded me that reproductive justice conversations are still based on bioessentialism, or the idea that a woman equals a vagina and a uterus and that reproductive issues are only women’s issues. My immediate response to both of these topics was pause.
When we say “abortion rights”, are we also including men and gender-diverse people that can give birth? Though cisgender women make up most of the population affected by this regressive abortion law, do the men and gender-diverse people also impacted not matter?
I can give birth, and many of my chosen brothers can too.
With abortion rights conversations almost always starring cisgender women—will we always be an afterthought? Will I always have to correct people in the grocery store, in classes, and in social justice spaces too?
Pause. I don’t subscribe to the idea of Lil Nas X being transphobic. I do, however, think that he did not foresee the inevitable transphobia that would ensue online. It was lazy of him to not acknowledge trans men and transmasculine people in at least a tweet after his album announcement.
A man being pregnant shouldn’t be a shocking gag. It’s boring. James Charles, Arnold Schwarzenegger, and Billy Crystal all have done it, and people have made jokes about men doing seemingly “non-man” things (like Martin’s Sheneneh and the L-Word’s lesbian man) for decades.
Some assumed that Lil Nas X’s “pregnancy” was just clickbait. Others questioned whether he knowingly made a choice that referenced trans manhood. We’ll likely never know his motivations, but what we do know is that Lil Nas X is a hypervisible Black gay man and most of these critiques came from non-Black people. In most cases, the same level of critique that was thrown his way is not duly given to non-Black people. And because Black people of all genders define so much of pop culture, it’s low-hanging fruit to bash Black celebrities when they make lazy choices.
So much of Black manhood is defined by hypermasculine presentation. Due to centuries of colonization, mainstream Black masculinity insists on being devoid of what we deem as feminine (dresses, emotions, and pregnant bellies). Is it a mix of all these things that make this anti-Black stew? Pause.
Multiple things can be true at once. Lil Nas X made an embarassingly cisgender marketing choice and men and masculine people being pregnant is not as normalized as it should be, therefore the sight of it is laughable to some of you. Anti-Blackness is cooked into the ways that Black celebrity is consumed and responded to.
A week of discourse on social media is everyday life for me. Being Black, trans, and masculine puts me in the dilemma of being both hypervisible and invisible every time I have to go to the bathroom or see a car with a siren attached to it. The erasure and mockery of Black transmasculine people that this concurrent discourse showed shouldn’t be treated as just another day on Twitter; it is a reality that my brothers and I live with. We have to reckon with the ways we treat Black transmasculine people like ghosts: denying our existence completely or treating our existence like a spectacle.
Abortion policies in the state of Texas affect folks of all genders. And worse, they’re coupled with anti-transgender and racist laws restricting education right now. In attempts to advocate for the marginalized, many contributed to a typical, limited view of the human experience. If our collective fight doesn’t at the very least include all bodies that can reproduce, with our bellies and humanity acknowledged, then we have already lost.
Clearly we have work to do. The question is will the rapture get here first.
Out with the Old: One Black Femme’s Struggle to Remove Their IUD

I’m a worrier, always have been. I overprepare for everything —I was even born a week early. As I’ve grown older and into my identities of being fat, Black, queer, nonbinary, and femme — I’ve learned that over-preparation is essential to my survival. After a pregnancy scare during graduate school, I threw myself into researching something more guaranteed than condoms. With school rapidly consuming my life, I needed something I didn’t have to constantly check in on; I wanted the Crockpot of birth control.
A friend of mine had told me about how much she loved her IUD, so I looked into it. I was hooked by the promise of long-lasting birth control with minimal maintenance. The procedure sounded simple enough: a doctor would insert a little hunk of plastic into my uterus, and five years later, I’d get it removed. Easy! At least, easier than reckoning with my lifelong needle phobia for the quarterly Depo-Provera shot, or the other popular long-lasting birth control Nexplanon, a matchstick-sized item fired into my arm, only to be cut out of me three years later. IUDs were the clear choice.

Although my decision was clear, I still agonized over IUD horror stories — perforated uteri, risks of the device expelling, and even becoming pregnant anyway — but the Mirena offered to stop my period altogether. I couldn’t pass it up. For years, menstruation fucked with my mental health and sense of self. Despite being terrified of the pain, I made an appointment to have an IUD placed. Anxiety coiled in my belly thinking of what could go wrong and was worsened by gynecological resources constantly tying birth control to cis womanhood and ignoring non-women like me. I tried finding better sources, but they were all by white, middle-class, cis women. I felt like an anomaly.
I considered skipping my appointment, but I couldn’t handle the threat of pregnancy again, so I went. The insertion itself was pretty standard. They measured my uterus’ depth, and an intense full-body cramp cracked through me. When they replaced the measuring tool with the IUD applicator, I was still too focused on the initial pain of measurement to feel the hurt of insertion — maybe that’s a small mercy. Afterward, the nurse gave me a pad big enough to ride home on. Back at my apartment, I crawled into bed, my poor uterus whimpering.
My periods never fully disappeared, but they did lighten significantly. Aside from checking the strings to ensure my IUD hadn’t rocketed out, I didn’t have any issues or think much about the small device inside me. By the time my T-shaped comrade’s expiration date arrived, I’d finished grad school, moved cities, and entered a new age bracket. With my periods becoming more irregular, I started researching replacements. The procedure was so simple that some go-getters had theirs replaced on their lunch breaks. I figured it couldn’t be any worse than the original placement, and I scheduled an appointment with Planned Parenthood. I’d never been to one before, and when I pulled up to the building a few weeks later, I wasn’t sure what to expect. I just knew I wanted the experience to be quick.
Thankfully, everybody at Planned Parenthood was so fucking nice. It was as good of an experience you can have when pulling out your vulva for strangers. I sent last-minute texts to friends letting them know I’d see them on the other side, and the nurse cranked me wide open with the tiny jaws of life. He grasped my IUD’s strings with forceps and pulled; I felt one dull cramp, then another. With the third cramp, he said, “It seems your IUD’s embedded. I’m not comfortable removing it because of the risks of infertility.”
Granted, I was there to become temporarily infertile — or at least temporarily hostile — but I appreciated his concern for my terrible, terrible womb. I rescheduled with the Planned Parenthood across town, where I was told they’d slather me with ultrasound jelly and guide out the device. I went home and worried I’d somehow caused this by not being careful enough. I scoured the internet for information on what to expect, but everything was either polysyllabic Latin or irrelevant, cheery articles, making me feel even worse. I just wanted someone to explain what would happen and provide reassurance that it wasn’t my fault.
There was nothing.

The night before my appointment, I was barely holding it together. Terrified at what could go wrong, I stayed up late trying to decipher complicated medical articles. When morning arrived, I was sleep-deprived and cranky getting into my Uber. We drove up to the building where a small group of protesters patrolled the sidewalks, demanding people like me be forced to carry children we didn’t want — they immediately cemented my decision to replace my IUD.
I checked in with the front desk, and after what felt like hours, a nurse called my name. We headed to the exam room where I laid on the table and of course, worried. What if they couldn’t remove my IUD and I’d have to spend the rest of my life carrying around this grim passenger? The gynecologist arrived, doing her best to put me at ease while reminding me to open my legs wider. She tugged on my IUD, but it held firm. “We’re going to give you some lidocaine,” she said, her smile pleasant. My heartbeat skyrocketed to rates you’d expect in someone being hunted for sport. I nodded weakly, preparing myself for needle horror, but it was just three tiny pinpricks, comparable to a mild period cramp. Soon, I felt absolutely nothing. They could’ve held a block party in there and I’d have no idea — it was incredible.
The gynecologist coated my FUPA with lukewarm ultrasound jelly; I could see my raggedy IUD on-screen, mocking me. While the gyno tried to wiggle out the device, she seemed to forget I was even in the room; it was just her and my uterus, locked in a battle of wits. I was window-dressing at best. That worked for me; the longer it took to remove my IUD, the more my dysphoria built. I felt invaded and on display. It took everything just to focus on breathing. She asked if I’d be comfortable if she applied more pressure, i.e. put her back into it; I gave a limp thumbs up. With some experimental angles, out popped my hormonal nemesis, gleaming underneath the hospital’s lights. “Would you like to replace your IUD?” the doctor asked. “It’s unlikely it’d embed again.” I paused, looking at the unopened Liletta box in her hands.
Even with the risk of repeating this entire process, nothing could ever be as painful as sitting alone and crying myself hoarse while waiting for the result of a pregnancy test. I didn’t want to be guilted into pregnancy by white evangelicals who’d destroy my child once they were old enough to be considered a threat. I said yes to replacing my IUD. I’m still a worrier but birth control offers me survival on my terms, and in a country hellbent on killing me — I’m not giving that up any time soon.
NY Needs More Midwives: Here’s How You Can Help
My mom remembers both times she gave birth with specificity. When she gave birth to my brother, she recalls, she felt much more prepared than with me, her first kid. Though she had practiced her breathwork for hours and hours, and was determined not to use any pain medication, and though my brother’s birth was shorter and easier than mine, still things didn’t go perfectly. What stands out to me the most about the story was who was in the room with her, and how they treated her. She described to me the midwife who was on her side, holding her hand, always keeping in mind and centering my mother’s birth plan – no meds. “You’ve got 14 contractions left! You can do it! Fourteen more minutes and you’re done!” the midwife coached her, gentle, encouraging, and empowering of my mother as she labored.
By contrast, the doctor who came in to supervise had his own agenda. My mother, even through the haze of pain and concentration as she strove to bring my little brother in the world, was able to register his arrogance. She remembers him breezing into the room with a small cup of coffee, insistently talking over her breathing, breaking her concentration to threaten her with his busy schedule. “I might get called away, so if you want medication, the time is now,” he said to her. She tried to wave him off, to get back into her mindset – fourteen more minutes! – but the damage was done, and the container the midwife had created for her, centered on my mother, her power, her plan, was broken.
The ending to my mother’s second birthing story was, still, a happy one. My mother lived. My brother was born, healthy and strong, and they both came home. For too many birthing people – especially Black birthing people – the story doesn’t end this way. In New York City, Black birthing people are twelve times more likely to die of childbirth-related causes than white people. (In the U.S. more generally, Black birthing people are two to three times more likely to die from birthing complications, according to BirthJusticeNow.Org, and the maternal mortality rate in the U.S. is twice that of other high income nations in the world.)
The disparities in health care for marginalized people in the United States, as well as gendered violence, are no doubt part of the cause. But I also keep coming back to the relationships among all the people in the room with my mother as she gave birth – the midwife, and the tradition from which she framed and understood birth and birthing people; and the doctor, with all the white supremacist arrogance and narcissism of the institution of Western medicine behind him, trained in a school of thought that calls him the expert and invalidates the agency and autonomy of the patients he is supposed to serve.
Not all midwives are the same, however; organizing around this very issue has been in the making for the past thirty years.
On June 10th, NY state senators will vote on New York Community Midwifery Bill S7078/A7898 to license Certified Professional Midwives and support Black and Indigenous birthing people in the state of New York.
Why is this important? I spoke to a dear friend of mine, Emily Varnam, who I’ve known within the sexuality education sphere for many years. She explained to me the difference between Certified Nurse Midwives and Certified Professional Midwives. It, like so many other issues within academic, medical, and social institutions, seemed mainly to me to be an issue that has to do with classism, racism, and elitism. Certified Nurse Midwives, Emily said, have to go to school for 5-6 years, and have to pay hundreds of thousands of dollars in order to be certified, something that often creates a barrier for Black and Brown prospective midwives. Certified Professional Midwives, by contrast, can learn to become midwives for much less money (around 20k) and less time. “It’s not that CPMs are less trained,” Emily emphasized, “It’s that they’re better trained for working out of the hospital” – and outside of the racist institutional practices that put Black birthing people at such increased risk. “CPMs are legal in 34 other states because they are considered experts, but not here,” she said. To not license CPMs in New York state “undermines their skills, and undermines the profession,” she continued.
Often when we consider education within the fields of mental health and physical health, we tend to think that more schooling results in more competent practitioners – and certainly, with the maternal mortality rate being so much higher for Black and Indigenous birthing people, we want the most qualified and competent practitioners out there. But consider how our medical system already fails birthing people of color – and is a functioning part of our other racist, violent systems, working the way they are intended to work. BirthingJustice.Org explains the link between medical racism and Black maternal mortality to the state sanctioned police murders of Michael Brown, Tamir Rice, Sandra Bland, Nina Pop, George Floyd, Breonna Taylor, and so many others. The same racism that results in police violence is baked into the medical institution itself, and we see it time and time again when doctors can’t recognize, or willfully minimize symptoms of illness when described by Black people, or when Black moms – even famous ones like Serena Williams – have to go above and beyond to advocate for the lifesaving care they need. According to Efe Osaren, a midwife-in-training I spoke to for this piece, “This bill is important for the district where we experience disparate birth outcomes, in part because of lack of access to appropriate midwifery care. This bill would improve access. Personally, it’s important to me because I’m training to be a CPM in another state right now and will be licensed this summer to hopefully work in my community in Brooklyn and create safe pathways for more Black Midwives.” (You can support Efe’s fundraiser for her midwifery training here.)
If the schooling necessary to become a Certified Nurse Midwife is prohibitively expensive for most BIPOC folks who want to be of service in this way, then what follows is similar to what you see in social work and therapy: a lot of white, privileged practitioners who have no connection to the communities they serve, and who will likely end up doing more harm than good. Additionally, cost is not the only factor that stands in the way of greater availability of Black midwives practicing from a holistic, indigenous traditions. “White supremacy is the educational barrier,” Emily told me. “Cost, yes, but largely even with the cost, the root of nurse midwifery is still slavery.” An article from the University of Virginia School of Nursing illustrates this history: “Until the late 19th century, the majority of births were attended by midwives, many of whom were Black, indigenous, or immigrant women. Most midwives, including enslaved women, drew upon traditional healing knowledge and practices passed down through generations. Others learned their practice through apprenticeship, either to local physicians or experienced midwives in their community. In the early 20th century, however, as childbirth became medicalized, physicians emerged as the primary birth attendants and childbirth moved from the home to the hospital.” And just like that, midwives went from being present to half of all births to being present as only fifteen percent.
By contrast, licensing more certified professional midwives means better access to care. According to @bxrebirthcollective,
“A CPM is a knowledgeable, skilled, and professional independent midwifery practitioner who is qualified to provide the midwives model of care.” Importantly, a CPM is trained in both in-hospital and out-of-hospital settings and can work in patients’ homes, or in birthing centers, which is part of how they create safer birthing experiences outside of the medical model especially for Black birthing people. The history of midwifery is centuries long; in fact, the advent of certified nurse midwives actually dislodged the historical position of midwives by creating nursing positions that were seen as subservient to the expertise of (mostly white male) doctors. According to the bill, “Midwives approach normal pregnancy and childbearing as natural physiological processes rather than as medical issues in need of intervention, and they are well-trained in identifying complications that could result in a different level of care being required. National evidence shows that when midwives are integrated into a state’s health care system, outcomes improve for birthing people and babies…[including] more vaginal births, including after cesareans; higher breast feeding rates; and higher satisfaction with care.”
In an essay in We Do This Til We Free Us, abolitionist Mariame Kaba often writes about the ways in which larger systems of oppression (institutions such as our legal system, academia, and the medical system, also known as macrosystems) are inextricable from the millions of smaller, one-to-one interpersonal relationships that, mosaic-like, contribute to the larger whole. This is what I see in my mother’s retelling of my brother’s birth – the doctor, a symbol and agent of white supremacist patriarchy, who had so little respect for the labor my mother was doing to bring my brother into the world, and so little humility for the immense power of her body as she gave birth. My mother, through the labor of her small brown body, giving form, sound, breath, and movement to the love, strength, power and sacredness of birthing bodies. The National Association of Certified Professional Midwives describes the importance of CPM thus: “The value of CPM is rooted in the belief in, and the commitment to, relationship and partnership with people having babies, to sharing power through shared decision-making, and supporting the childbearing person’s experience of control.”
As Efe said, “When Black women are safe, everyone benefits.” Reconnecting us to our sense of control – of our agency – is an integral part of trauma healing work. It’s on my mind a lot as a therapist, and the ways in which systems of oppression are enacted on our minds, bodies, and spirits, both in how we interact with institutions, and the ways in which we interact with each other, are things that we have to grapple with in our efforts toward undoing our current system and building a newer, more just world. The violence against Black and Indigenous birthing people is intergenerational violence and trauma happening in real time, in each birth. Healing it – by making midwifery more accessible for more people, in the contexts and environments that are centered on the comfort, care, respect, and empowerment of birthing people – is one deeply important step forward in creating that world.
How You Can Help:
Call or Email the following script (from @bxrebirthcollective):
Hello my name is [INSERT YOUR NAME] and I am your constituent from [INSERT CITY AND STATE]. I am calling to ask you to support the Community Midwifery Bill (Bill Number S7078/A7898). New York is in an ongoing maternity care crisis that disproportionally effects Black birthing people. Licensing community midwives is an important step in addressing this and providing more care options in New York.
As a [PARENT/BIRTHWORKER/CONSTITUENT] I urge you to co-sponsor the Community Midwifery Bill (S7078/A7898). Black maternal health and birth justice advocates support this bill and encourage you to do so as well. Thank you.”
Share the bill:
Follow and Share from @nycpm.inc
Use the #hashtags:
#NYCPM
#CommunityMidwiferyBillNY
#YesOnS7078
#YesonA7898
#NYNeedsMoreMidwives
Is Vaginismus Making Penetration Painful? Here’s What It Is and How to Treat It
If you experience severe pain during vaginal penetration or if you just can’t seem to get anything in there, then you might have vaginismus. This condition causes involuntary muscle contractions in the vagina before or during penetration, making penetration difficult or even impossible. These contractions can get in the way of certain practices and pleasurable activities, like penetrative sex, penetrative masturbation, inserting tampons on menstrual cups and receiving pelvic exams. But with the right guidance from a doctor and/ or a physical therapist, vaginismus can be treated.
What Causes Vaginismus?
Experts speculate that a variety of factors can lead to vaginismus, but like most conditions that affect vaginas, the precise cause of vaginismus is grossly under-researched. People with primary vaginismus have never been able to experience vaginal penetration, while people with secondary vaginismus developed symptoms later in life. Sometimes vaginismus occurs in response to a physically and/ or emotionally traumatic event, like sexual assault, childbirth or a surgical procedure, but sometimes the symptoms can pop up without a known cause. It’s estimated that up to 17% of vagina-owners experience vaginismus, but given that the stigma associated with the condition (and with vaginal health in general), some experts believe that the actual numbers are much higher.
What we know for sure is that once a person has vaginismus, the muscle contractions can feel impossible to control. Dr. Anna Yam, PhD, a clinical psychologist who specializes in pelvic pain, told Bustle that the muscle contractions associated with vaginismus are similar to an eye blink. Think about it like this — if an object is moving towards your eye, you instinctively blink to protect yourself. The same thing happens with vaginismus. If you’ve experienced painful penetration, your body perceives any penetration as a threat, so your muscles involuntarily contract to prevent the pain from happening again. As Dr. Yam explains, “Biological muscle contraction is reinforced by the psychological fear, and vice-versa.” Without treatment, this cycle can cause people to suffer from vaginismus for years or even for a lifetime.
How Is Vaginismus Diagnosed?
Gynecologists can diagnose vaginismus after listening to a patient’s symptoms and performing a pelvic exam. Unfortunately, not all doctors understand this condition, and some people struggle to get an accurate diagnosis. Some people with vaginismus have been told to “use more lube” or “just have a glass of wine and relax” when they tell their doctors about their pain. If you experience pelvic pain and your doctor doesn’t take your symptoms seriously, find another practitioner who can give you the kindness and care you deserve.
Why Treat Vaginismus?
Much of the writing about vaginismus is 1.) Directed at straight, cisgender women and 2.) Steeped in the false narrative that “sex” equals penetration. Unless you’re trying to get pregnant, penetration isn’t a necessary part of a healthy, fulfilling sex life. But if you think you might have vaginismus and you’re curious about the pleasures of penetration, then that’s a totally valid reason to seek medical help.
Even if you’re not trying to get pregnant and don’t want to add penetration into your sexual repertoire, there are other reasons to get some answers about your pelvic pain. While vaginismus isn’t directly life-threatening, some other conditions that cause pelvic pain are, so it’s important to get your vaginal health assessed by an informed, attentive medical professional. Additionally, some of the problems associated with vaginismus — like not being able to receive regular pelvic exams — make it hard or impossible to track other aspects of your reproductive health. Sometimes gynecologists can find ways to perform pelvic exams that are more comfortable for people with vaginismus, but if your muscle contractions make penetration impossible, treating vaginismus can help you tolerate pelvic exams and stay full informed about your well-being. If your doctors can find safe and effective ways to perform pelvic exams if and when you need them and if you don’t have any other reason to include vaginal penetration in your life, then you don’t have to treat vaginismus unless you want to.
How Is Vaginismus Treated?
If you’re experiencing vaginismus in response to a traumatic event, therapy is probably an important tool for your healing journey, but it isn’t going to stop those involuntary muscle contractions. For that, you’ll need to retrain your pelvic floor. The most common course of treatment for vaginismus is the use of dilators, or a series of dildos that range in size. Most doctors have their patients begin with inserting a very slim dilator while lying comfortably on their back at home. The dilator should be left in for whatever amount of time has been designated by your doctor (usually around twenty minutes) before it is removed. Patients are asked to repeat this practice daily, moving up a size when they’re ready.
The regular use of dilators creates new muscle memories, helping your body understand that penetration is not a threat. After regular dilator use, people with vaginismus can have better control over their pelvic floor muscles, preventing the involuntary contractions that prevent or complicate penetration.
In some cases, you might need to see a pelvic floor physical therapist in order to make a full recovery. A pelvic floor physical therapist can use exercises and internal massage to relax and retrain your muscles. The idea of a stranger massaging the inside of your vagina might sound a little strange, but pelvic floor physical therapy is extremely effective. In addition to treating vaginismus, pelvic floor PT can help all kinds of pelvic floor conditions, including pelvic floor weakness, constipation, vulvodynia and endometriosis. Additionally, physical therapists typically spend more time getting to know their patients than doctors, so a PT might be able to better understand your history and provide more individually-tailored care.
How Do You Psychologically Heal From Vaginismus?
If you’re experiencing vaginismus, you’re not broken. Vaginismus is your body’s way of protecting you from pain — your muscles are just overdoing it. But even if you have all of the facts, vaginismus can be hard on your mental health and your relationships. In addition to the physical pain, people with vaginismus often experience anxiety, shame and isolation. Once you associate certain sexual activities with pain, it’s hard to experience sexual pleasure with a partner or by yourself. Some people with vaginismus find themselves avoiding sex entirely and worry that they’re disappointing their partners, even after they’ve recovered from the disorder. If you are living with pelvic pain and you’re struggling with any of these feelings, talk about it with a therapist, your partner(s) and other people you trust. Physically and mentally healing from vaginismus is possible if you’re willing to open up and get the support you need. And once you start talking openly about your experiences, you might find that some of your loved ones are dealing with similar symptoms. Vaginismus and other pelvic pain disorders are more common than most of us realize — they’re just not openly discussed.
How 2021 (and the Biden/Harris Administration) Could Mark a Turning Point for Reproductive Rights
Last year concluded with a monumental victory for human rights, when Argentina legalized abortion thanks to decades of grassroots organizing. And as early as this month, the US could turn over a new leaf for reproductive rights with the inauguration of the Biden-Harris administration, following a Trump era defined by an unprecedented surge in political attacks on the state and federal level. Throughout his presidency, on top of emboldening extremist state lawmakers and gutting funding for health care, Trump repeatedly used his platform to conflate abortion care with murder.
Already, the incoming administration has pledged to be a friendly one for reproductive rights. But to meet the urgency of this moment as we mark 48 years of Roe v. Wade on Jan. 22, we need more than friendliness. We need proactive policymaking to ensure pregnant people can get the real-life health care and supports they need, with a judicial landscape increasingly stacked with anti-abortion extremists, and state legislatures that have wasted no time introducing and passing punishing and restrictive bills in the first weeks of 2021.
The Biden administration’s early promises include reversing the Trump administration’s global gag rule policy, enacted in the first days of his presidency in 2017, which prohibits federal funding from supporting abortion and reproductive health care as well as sexual health education abroad. Increased maternal mortality rates and child marriage are historical consequences of such policies. Biden and Harris are also expected to restore Title X funding, which funds family planning for people who rely on Medicaid. The Trump administration had diverted Title X funding from clinics offering sexual and reproductive health care to predatory “crisis pregnancy centers,” and dangerous abstinence-only programs, resulting in the closure of several clinics.
The Trump administration rationalized defunding Title X by asserting that some clinics that receive funding offer abortion services, despite how the Hyde Amendment has prohibited federal funding from covering abortion care since 1976. The incoming Biden administration has also pledged to lift Hyde, which effectively prioritizes the personal and religious views of a narrow minority of abortion opponents in the country over the health and autonomy of everyone else. This policy position by President-elect Biden is a consequence of aggressive pressure from advocates in 2019, when he initially expressed support for it.
These are promising policy positions from the president-elect, who formerly limited his plans to “codifying Roe v. Wade” while on the campaign trail. But while formally protecting the legal right to abortion in the event that the 6-3, anti-abortion Supreme Court reverses it in the near future, advocates and people who organize for real-life abortion access on the ground have emphatically told us for years that too many barriers already exist, even with the legal right in place. All of these barriers carry the most harm for people of color and LGBTQ people, who are more likely to struggle to afford care, or have to travel across state lines to access it.
Especially during the pandemic and economic recession, both of which have created new barriers and new opportunities for states to block care, the federal government can’t be complacent. Following a recent Supreme Court ruling that blocked telehealth options for obtaining medication abortion care, the Biden administration will have to act quickly to lift medically unnecessary restrictions and ensure people can still get the care they need from home during a pandemic that grows deadlier by the day.
Access to medication abortion pills was especially important in the early months of the pandemic, when nearly a dozen states tried to exploit it to halt abortion services by falsely labeling it “non-essential” health care. But being forced to carry an unwanted pregnancy is a time-sensitive medical emergency, which anti-abortion politicians at the state level have long treated with inhumane and dangerous legislation to delay or deny access to care altogether. In recent years, states have passed and even enacted laws ranging from six-week abortion bans, citing pseudoscience about “fetal heartbeats,” to abortions later in pregnancy, which are often necessary for extreme health circumstances or delays in care due to restrictive laws. More recently, Ohio’s governor signed a bill to require people who have abortions to pay for the burial or cremation of their fetus. The law would also result in death certificates for aborted fetuses, which could soon make patients’ abortions public record.
The surveillance of people’s abortions and pregnancies is a mounting trend we’ll likely see more of in 2021, especially following a recent uptick in people being criminalized and even jailed for miscarriages, stillbirths, and self-managed abortions with abortion medication. Recent research has shown nearly a third of early abortions are medication abortions, which involve inducing a miscarriage, and this number has likely increased during the pandemic as more and more people opt to induce abortions at home.
Laws that ban, restrict or stigmatize and treat abortion and pregnancy with suspicion contribute to a culture where the health service is more likely to be criminalized. The incoming administration could take decisive action to curb these restrictions with a plan that Vice President-elect Kamala Harris formerly proposed on the campaign trail, which would require states to get pre-clearance from the federal government before implementing more abortion-based restrictions.
Ultimately, the future of abortion access and safety from criminalization could rest largely with the courts, from the Supreme Court to Circuit Courts across the country. While Biden has pledged to exclusively appoint Justices who would respect abortion rights, following a Trump presidency that yielded more confirmed judges and Justices than any presidency in recent history, this pledge isn’t enough. Only court expansion can begin to give abortion access and other issues crucial to the health and autonomy of people of color, pregnant people, LGBTQ folks, and immigrants a fighting chance, following years of the minority party stealing seats and rushing the confirmations of unqualified extremists.
Amid a public health crisis and following the ousting of a presidential administration that leaves an enduring legacy of violence targeting pregnant people, we can’t have a passively “pro-choice” White House and Congress. The moment we’re in requires bold action and bolder policymaking from the incoming administration on day one, from funding reproductive health care on the federal level, to proactively reining in state-level attacks. And the recent victory for abortion rights in Argentina models just how to achieve this: through relentless grassroots organizing and pressure on our state and federal representatives.
Worried Your Vote Can’t Protect Reproductive Rights? Mutual Aid Can (and Does)
Four years since the election of President Donald Trump, the worst fears of reproductive rights advocates were seemingly realized with the confirmation of Amy Coney Barrett to the Supreme Court, cementing a 6-3 anti-choice majority to gut access to reproductive care and potentially even criminalize abortion. Naturally, Barrett’s confirmation was followed by reinvigorated calls for voting as the sole solution to the crisis we now face, to prevent even more dangerous judicial appointments on the federal level, and abortion bans on the state level.
Voting can serve as critical damage control — we know a President Joe Biden would support funding for reproductive care and appoint only judges and Justices committed to reproductive rights. And up and down the ballot, plenty of candidates and ballot measures go beyond reducing harm and make real, positive change, especially on the local and community levels.
Yet, many of the crises we’re being warned about with this new 6-3 conservative Supreme Court majority — discrimination against LGBTQ folks, people struggling to afford health care if the Affordable Care Act is gutted, and, certainly, people not being able to have abortions — already exist. From abortion funds, to legal defense funds, to mutual aid networks, the solutions already exist, too, due to the work of people who have long felt their communities are left behind by elected officials, and denied the full actualization of long-standing legal rights.
Across the country, mutual aid networks have long put in the work of moving wealth, and creating funding and logistical arrangements for people to afford abortion care and contraception, as well as transportation, lodging, and child care to reach these resources. In a country where 90 percent of counties lacks an abortion provider, funds have created the infrastructure for low-income people to cross abortion deserts, or regions where one clinic serves over 100,000 people of reproductive age. Some funds have even created special resources for trans people who face added barriers to reach abortion and other sexual and reproductive health care, as well as legal support and other resources for minors and young people to get care, too.
Abortion funds across the country last year supported 56,155 people seeking care, all amid a backdrop of unprecedented state-level abortion bans and restrictions being passed. Several funds in different states reported collaborating to help people travel across state lines to get care, and for funds in some regions, the majority of clients served were people of color. Throughout the crisis of COVID-19 this year, funds have spoken out about how much more urgent their work has become, especially as more people have lost their jobs, savings, or insurance, and all the existing barriers to get care have only worsened.
Groups like this have existed since before Roe v. Wade was decided in 1973, and adapted their work to new political realities following the decision, through bans on coverage of reproductive care, rampant legislative attacks and closures of clinics, and even the continued criminalization and punishment of people who have abortions or lose their pregnancies, and need legal support. Amid COVID-19 and the shuttering of clinics across the country in recent years, community advocates and aid networks have helped educate and facilitate crucial access to abortion pills, which are FDA-approved and allow people to safely end a pregnancy at home without the necessity of traveling to a clinic.
Mutual aid and community care have always existed as a response to the devastating inevitability of state violence. After all, state violence is more than incidents of racist police brutality — it also encompasses the government’s failure to ensure access to basic resources like health care and especially reproductive care, most often for the poor and communities of color. State violence certainly encompasses government policies that deny people bodily autonomy and coerce their pregnancy and reproduction. The inextricable connection between violence and the state, especially for people of color, has led many to be dubious about looking to the state and elections for easy solutions, and instead, create solutions in their own communities outside of the government.
Because of these long-standing mutual aid efforts, the infrastructure to address the crises we face today is already there. To make a real difference, we should invest in what already exists, and the people and groups who have been doing the work.
Following the confirmation of Barrett to the court, like we saw after the confirmation of previous Justices who threatened Roe and other human rights, many social media users shared plans to hoard emergency contraception and birth control pills, or start crowdfunding for others’ abortions and travel across state lines, as well as legal fees if needed. But rather than personally try to reinvent the wheel and divert attention and resources from people who have long been doing the work, we should listen to their expertise on how we can support the work they’re already doing.
And for starters, on top of financially contributing to and volunteering with funds and other mutual aid networks, we could also simply not hoard basic resources like Plan B, which already can be costly and inaccessible, and would become even more so in scarcity.
Participating in elections, and especially elections like this year’s, will always be critical to the fate of the country and its most marginalized — after all, elections and voter suppression are what pushed us to this very point of reckoning. With the Supreme Court poised to potentially uproot life as we know it in America, voting by itself might fix some things, but it can’t fix everything.
Investing our money and effort into community care can go further than just relying on elections and institutions that have always upheld a status quo of oppression. None of us can do everything, or single handedly ensure everyone gets the care they need — but we can all find and contact our local funds, and learn about ways to volunteer, either for their hotlines, or to help with transportation, lodging, child care, fundraising, and other needs. We have to do more than put all our faith into a system that’s working as it was designed to marginalize women, people of color, and queer and trans folks. Instead, let’s recognize the transformative power and potential of mutual aid and direct action, starting in our communities.
AS Politics Survey: LGBTQ Health Care & Amy Coney Barrett’s Impacts
As we head into the 2020 election, our contributing data brain, Himani Gupta, is analyzing data from past Autostraddle surveys to find out what issues are most important to our community and what is currently at stake.
In this week’s Senate confirmation hearings, Amy Coney Barrett’s reticence to talk about her positions made it pretty clear how much damage she plans to do once she gets to the Supreme Court. Among the many disturbing things we know about Barrett’s political views, her stances on several health care issues are going to inflict a lot of harm on a lot of people.
Autostraddle’s Politics Survey, launched in December 2019, asked about a number of topics related to health care, namely: religious freedoms, reproductive rights and the affordability of care. At the end of July, I followed up with some of the original survey respondents to see if anything changed in terms of how they thought about the affordability issues in the wake of the pandemic.
We’re going to look at just how important these issues are to our community and discuss what’s at stake with Barrett’s impending nomination to the Supreme Court.
Who Took the Politics Survey
Before we turn to those results, we need to start by understanding who took the Politics Survey and who participated in the follow up.
The Politics Survey was available for anyone to take on Autostraddle’s website between December 3, 2019 and January 10, 2020. Over 4,400 people started the survey and just over two thirds made it to the mandatory questions on gender identity and sexual orientation. The analysis is restricted to queer people who identified as women, non-binary and/or trans, which gives us our sample of 2,834 respondents.
At the end of July, I reached out to the 994 Politics Survey respondents who said they were open to being contacted for follow up. Between July 26 and August 16, 662 people completed the Follow Up Survey. This divides our original sample into two subsamples: people who took the Follow Up Survey and people who didn’t.
For the most part, the Follow Up Survey respondents are a similarly diverse group of people compared to those who didn’t take the Follow Up Survey. A slightly greater proportion of trans women and non-binary women took the Follow Up Survey. The gender identities and sexual orientations of respondents to both surveys are shown below.

While the two subsamples are similar in terms of race/ethnicity, disability status and age, they differ on education. As shown in the figure below, more of the Follow Up Survey respondents earned a bachelor’s degree as their highest degree.
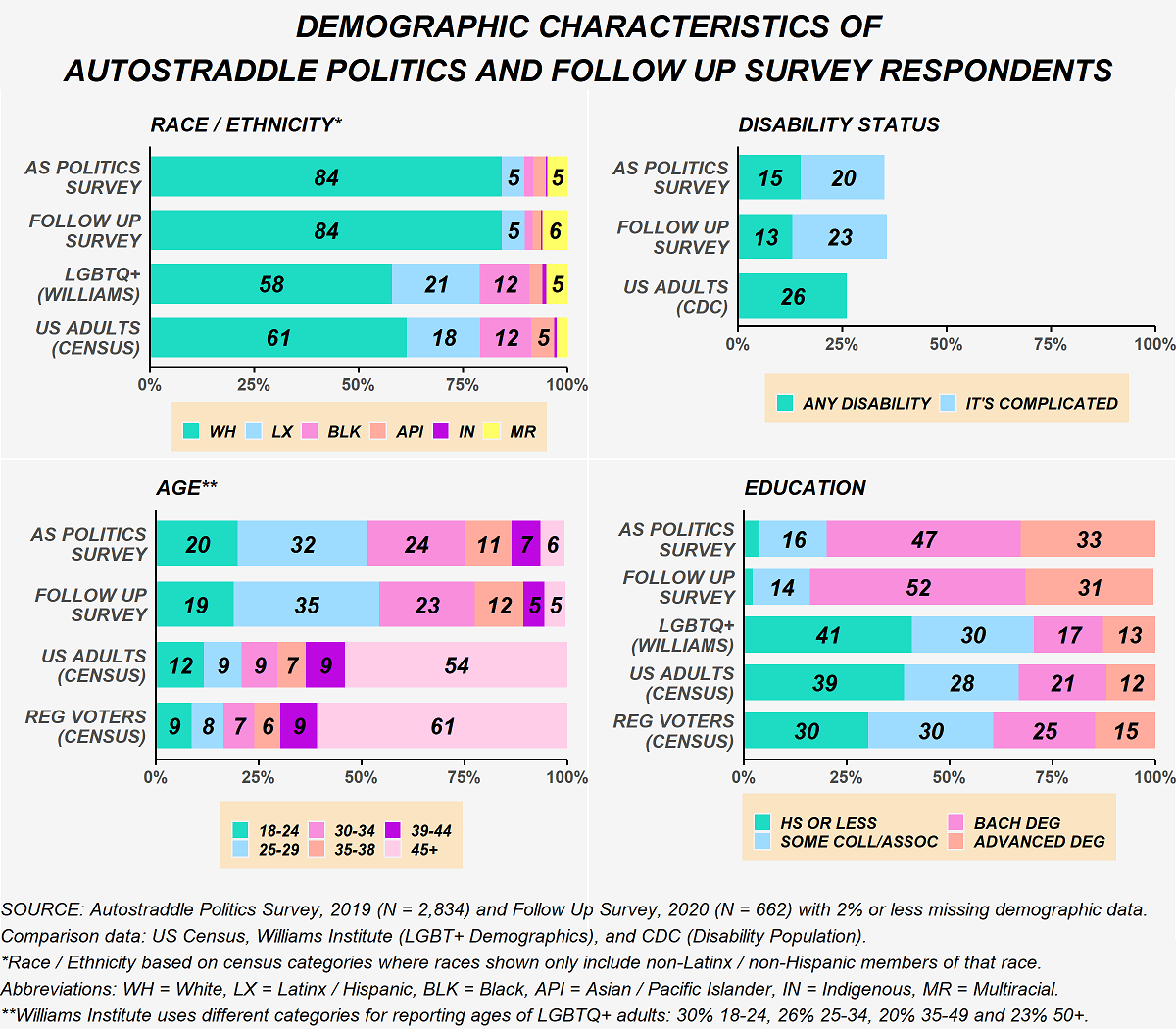
Another key difference is that fewer people living outside the U.S. participated in the Follow Up Survey. As a result, more of the Follow Up Survey respondents are registered to vote in the U.S. Once we account for this difference, the two subsamples are similar in terms of what region they live in. They also live in similar types of places, generally. (Note that the U.S. Census uses “urbanized clusters” and “urbanized areas” in its data collection, which are very different from how most people think about urban and suburban.) In terms of income, there is some variation, even after accounting for the differences in the proportions of non-U.S. residents.
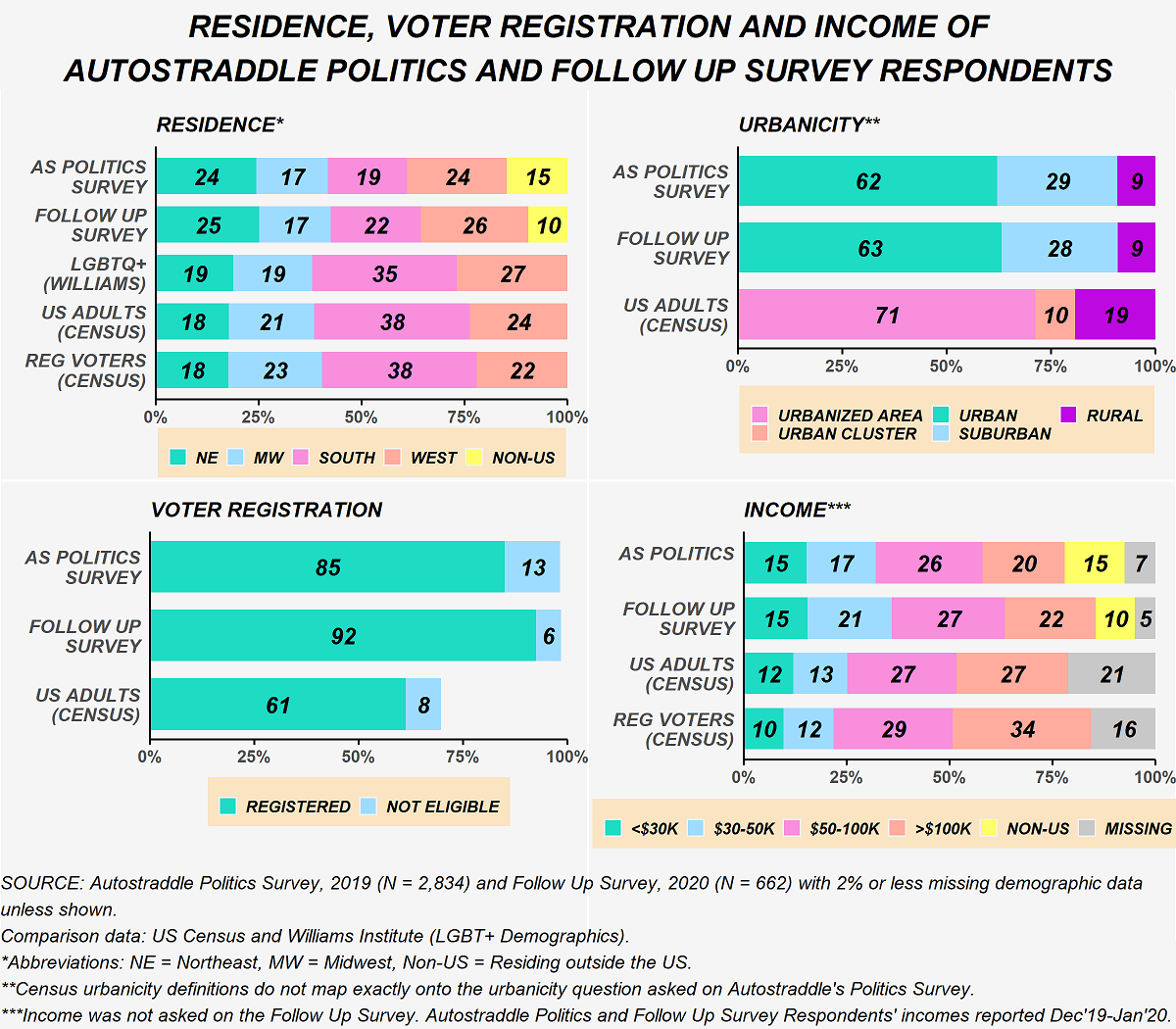
There are, of course, unmeasurable differences between the type of person who would complete a second political survey and the type of person who wouldn’t. That being said, the Follow Up Survey provides important insight into shifts within our community.
“Anyone Who Would Discriminate ‘Based on Their Religious Beliefs’ Should Not be in Health Care.”
Far too often religion becomes the justification for mistreatment in health care, particularly when it comes to LGBTQ+ friendly and, especially, trans-inclusive care and reproductive rights. Based on a poll conducted by The Economist/YouGov in October 2019, Americans are conflicted in their views on a government regulation allowing medical providers to deny services because of their religious beliefs. Those divisions are largely along partisan lines with 81% of liberals opposing such a measure compared to 55% of conservatives supporting it.
Autostraddle Politics Survey respondents were in resounding opposition. Going beyond that question, several people further emphasized in free text comments that providers who have religious qualms about providing services should not be working in health care.
The figure below compares the results from the Politics Survey to the Economist/YouGov poll.

While the topic of religious freedoms in health care specifically didn’t come up in the confirmation hearings, Barrett’s views on religious freedom more broadly are well established. Earlier this week, writers for the Washington Post laid out Barrett’s disturbing history of supporting “preferential treatment” for religious expression. It’s likely, based on her record, that if a case on religious freedoms in health care were to make its way to the Supreme Court, she would rule in favor of those who are denying health care.
It’s also very possible that a case on this exact issue will make its way to the Supreme Court soon. In May 2019, the Trump administration created “conscience” protections that would prevent health care institutions from accessing federal funds if they took disciplinary actions against health care workers who denied services because of their religious beliefs. A few months later, in November of that year, a federal judge struck down the rule.
Anti-Trans Discrimination In Health Care Was Already A Big Problem. And Then the Trump Administration Intervened.
The Politics Survey asked respondents if they had been denied health care because of their gender identity or presentation. Among the overall sample, 5% of respondents said they had been denied services and 8% said they were unsure if that had happened to them.
But those overall numbers mask a deeper story. The figure below shows the stark differences in responses to the question on denial of services by the gender identity of the survey respondent. 50% of our trans women respondents had either been denied services because of their gender identity or presentation or had an ambiguous experience along those lines. About a third of our non-binary respondents shared that experience as well.

In addition to the responses shown above, several people shared other negative experiences in free-text comments, such as being discriminated against in other ways, traumatized and mistreated by trans-incompetent health care providers. Others mentioned putting off health care to avoid mistreatment and discrimination.
In an effort to address some of these issues, in 2016 the Obama administration implemented anti-discrimination protections on the basis of gender identity. In June of this year the Trump administration eliminated those protections. Mere days later, the Supreme Court issued its landmark ruling in Bostock v. Clayton County. In the majority opinion, Justice Neil Gorsuch wrote that discrimination against trans people qualifies as “discrimination on the basis of sex.” Although that case was dealing with employment protections in the Civil Rights Act specifically, the same logic applies to a whole swathe of other legislation, including the Affordable Care Act. In fact, in August, a federal judge struck down the Trump administration’s attempt to end trans health care protections, citing the Bostock decision.
It seems almost inevitable that trans health care protections will find themselves before the Supreme Court sooner or later. And while Barrett’s views on the rights of trans people did not come up in the confirmation hearings, her use of the term “sexual preference” when asked about LGBTQ+ protections speaks volumes about how she views the community as a whole. Though she later apologized for using the term, her ties to a law firm that has fought to legalize discrimination against LGBTQ+ people have also been reported this week.
Reproductive Rights Have Been Steadily Eroded for Decades.
Even before Barrett was nominated, the alarms were sounding that Roe v. Wade would be effectively gutted by a Supreme Court with a conservative-majority. In many ways, it already has been. Abortion is such a hot button issue that any law that gets passed, whether at the state or even a long-shot attempt in Congress, inevitably will make its way to the courts and, often, up to the Supreme Court. That small handful of people wields an incredible amount of power when it comes to reproductive rights.
Barrett’s views on abortion are clear. She has a long history of explicitly opposing the right to choose. Yet, when directly confronted on the issue during the Senate confirmation hearings, she, unsurprisingly, punted, claiming she would not be going in with an “agenda.” I’m not sure how someone who sponsored a “right to life” ad in 2006 can claim to not have an agenda on this topic.
Respondents to Autostraddle’s Politics Survey could not be farther from Barrett in their views. There was near unanimous support for abortion with almost 90% supporting that basic right to choose in all circumstances and another 10% wanting it to be “legal with limitations.” That was, more or less, consistent no matter how I sliced the data. In contrast, a Monmouth University poll from June 2019 found that while nearly two-thirds of American adults want abortion to be legal in some capacity, only 29% fully support it in all circumstances. The figure below compares these results.

The High Cost Of Health Care Hits Our Community Particularly Hard.
Alongside these battles over what medically-necessary services are legally permissible is the fight over the prohibitively high cost of health care. A well-established problem nationally, this is another aspect of the health care system that especially harms our community. The Politics Survey asked whether respondents to indicate whether they or someone in their household had forgone needed services because of they could not afford them. Results from the Politics Survey are compared to a Monmouth poll conducted May 2019 in the figure below. Note that all results discussed in this section exclude Politics Survey respondents who live outside the U.S. because of the policy-specific nature of this issue.
Once again, the overall numbers hide a deeper story. The Monmouth University poll found substantial differences in the response to this question by income, which is unsurprising given that cost is the underlying issue. A similar pattern was observed among Politics Survey respondents, as well. This comparison is shown in the graphic below.

A direct consequence of these disparities in access to care by income level is disparities in access to care by other demographic characteristics that are correlated with income, including gender identity, race/ethnicity and disability status. So while the rate of forgoing health care because of the cost among our community as a whole is 63%, among trans women and non-binary people that rate is 70% and 73% respectively, among Black and Latinx people it’s around 70% and among people living with disabilities it is a galling 78%. Health care is just one more arena where some of the most marginalized members of our community face the dual threats of identity-based discrimination and poverty.
The Growing Appeal of Medicare for All
Several policy ideas have been floated in the last few years to address the high cost of health care. A single public plan like “Medicare for All” has gained substantial traction on the left and dominated much of the conversation during the Democratic primaries. Among Politics Survey respondents, over 80% wanted to move towards a universal public system either immediately or eventually. The American public, of course, is much more divided. The figure below compares responses from the Politics Survey to a Monmouth University poll conducted in August 2019.

Support for a single payer was substantially higher among Politics Survey Respondents than U.S. adults, regardless of income. But, nonetheless, a greater proportion of our lower income respondents wanted to move towards a universal public system at some point than our higher income respondents: 88% of respondents with an annual income below $30,000 compared to 78% of respondents with an income above $100,000. There wasn’t much variation in support for Medicare for All by gender identity, race/ethnicity or disability.
I was curious to see if the pandemic led to any shifts in how people viewed Medicare for All, so this same question was asked on the Follow Up Survey. Among the people who took the Follow Up Survey, support for moving to Medicare for All at some point stayed about the same. The urgency, however, changed. In the Politics Survey (conducted December 2019 – January 2020), 70% of Follow Up Survey respondents said they wanted to get rid of all private insurance compared with 14% who preferred an opt-in with eventual transition to single payer. By the time of the Follow Up (conducted July – August 2020), that had shifted to 77% and 9%. The change is modest but not statistically significant.
The Supreme Court Could Affect Single Payer Health Care in Many Ways
One of the drawbacks of a single payer public health plan is that, depending on who’s in power, it might not cover politically divisive but medically necessary procedures like hormone therapy, gender reassignment surgery or other trans-inclusive care, contraceptives or abortions. If recent history is any model, it’s fair to assume that even if Democrats managed to pass a plan like Medicare for All that covered all of these things (more on that in a minute), private companies would start suing left and right and the matter would make its way to the Supreme Court. Conservatives on the Court have already proven that they will side with religious freedoms at the expense of contraceptive care, as we saw in Burwell v. Hobby Lobby. All evidence suggests they would act exactly the same way if there were a single payer law with a mandate for covering trans-inclusive care or abortions. And we know Barrett will fall even farther to the right on this than the conservatives currently on the Bench.
In addition to legal scrutiny over what could be covered in such plan, a single payer plan will very likely find itself in court for mandating health coverage, the way the Affordable Care Act has on multiple occasions. Here again, history is instructive of what the future may hold. In 2012, the ACA was narrowly saved with Roberts writing the majority opinion. As a legal scholar explained in a recent interview with The New Yorker, a key issue in that case and the one that will be heard by the Court the week after the election is whether requiring people to purchase health insurance is “an unconstitutional act of coercion.” In the 2012 case, Roberts ruled that the ACA, specifically, was not because of the fines imposed on people who did not purchase health insurance (which Roberts viewed as a “tax” and therefore under the purview of Congress). After Republicans did away with the fines in 2017, the latest challenge to the ACA argues that the current form of the ACA is now coercive.
Many are concerned that Barrett’s hasty nomination to the Court will be the end of the ACA once and for all (a Republican dream and Trump campaign promise). In the hearings, Barrett, of course, punted on the issue, but she has previously criticized Roberts’ 2012 opinion that saved the ACA.
It’s hard not to imagine that all of this would replay itself in one form or another if a public, single payer plan were to somehow become the law. Once again, the Supreme Court has tremendous power in determining the shape of health care in this country.
Biden, of course, does not support single payer, though Harris did during the primary. As the pandemic has worn on, Biden’s moved closer and closer towards it. In July, a “unity task force” between the Biden and Sanders campaigns put forward a plan to expand health care access substantially. While not single payer, the plan will lower the qualifying age for Medicare and includes a government-run public health insurance option. That public option would be available to anyone but would automatically enroll low-income people who lose their jobs. Again, what a conservative court will do with such a law remains to be seen.
Is Everything Doomed?
Barrett will be confirmed before the election. Republicans are bending every rule and norm to make that happen. We will have a 6-3 conservative majority on the Supreme Court in a matter of weeks. Roberts’ seemingly liberal sleight of hand votes that have, bit by bit, undermined policies that enshrine basic rights will no longer put off the inevitable. So where do we go from here?
The only say we have over who’s on the Supreme Court is through who we vote into office in the Senate and the Presidency. For his part, Biden continues to dodge questions about court-packing, which leaves us with something to hope for. Last week, Natalie covered the close Senate races; If you have the money or the time, donate to and volunteer to campaign for those races. And after the election, the phones need to start ringing.
Extra! Extra!: What Would Happen If We Did Lose Roe v. Wade? Let’s Talk About It
This week has been incredibly difficult. From Ruth Bader Ginsburg’s unexpected death last Friday to the Kentucky grand jury decision on Wednesday that brought no charges against the three men who murdered Breonna Taylor, I know I personally reached a point where I just could not read the news.
I simply don’t have the words to talk about Ginsburg’s passing. (Riese wrote a beautiful tribute to her last week.) In terms of the political implications, well the headlines alone are enough. McConnell is unsurprisingly immoral. We liberals were a bunch of fools for briefly pinning our hopes on Mitt Romney. And I cannot even bear to get into the long list of policies that are about to be gutted. The consequences of this are monumental. At the same time, a woman I really admired and respected also just died.
And then there was the verdict in Kentucky. Again, I find myself at a loss for words. Truly, all I can muster is, “for shame, America, for shame.” As I’ve said before, every single time this happens I think about the endless list of names that I do not know, people who were killed wrongfully at the hands of the police and vigilantes, who never, ever get anything even close to resembling justice. Breonna Taylor’s case was stunningly clear. A woman was killed in her sleep. How hard is it to recognize that this was wrong? But, as Fabiola Cineas writes for Vox, as Black people know all too well, “This is how the system was designed.”
So this week’s Extra! Extra! turns to other areas of the news. Not because RBG’s death and the verdict on Breonna Taylor’s murder aren’t important. But because sometimes things are so strongly felt, no words could possibly capture their lasting consequence. We turn instead to several trans rights issues, reproductive rights, some disturbing trends on the far right and an update on how COVID-19 is upending this country. To close out, a few stories of small wins, a little bit of hope.
Trans Rights
The long history of trans voters’ disenfranchisement, explained
The Accelerating Attack on Trans Student Athletes
Lawmakers push schools to consider transgender sports policy
GOP Senator introduces bill that could require genital exams for girls competing in school sports
Himani: This summer saw a landmark ruling for trans rights. And at the time, Natalie, quite presciently, wrote:
I’ve heard from a lot of people — far more adept at these issues than me — that the Court’s decision in Bostock undermines the administration’s anti-trans efforts, including last week’s rule change by the Department of Health and Human Services. I suppose my question then is: what does that look like, in practice? Will HHS or HUD withdraw their efforts on their own accord or will groups have to prepare for years of litigation to ensure that our lives are free from discrimination?
Well, here we are, just three months later and as Natalie foresaw, there’s no way that ruling alone will stop a government that is hellbent on denying trans people civil rights. As Melissa Gira Grant writes for The New Republic regarding the Bostock ruling, “A win there can’t provide trans people the resources to take on multiyear anti-discrimination cases. Oftentimes, as we have seen with abortion rights, a big win just emboldens the opponents of a given right to escalate their attacks elsewhere.”
Betsy DeVos is the latest in the Trump administration to take up the anti-trans mantle. Squarely defying the implications of the Bostock ruling, her administration is arguing that schools that allow trans girls to participate in sports are breaking federal anti-discrmination laws. Citing the pending case between the Department of Education and Connecticut, state officials in South Dakota are now pressing the South Dakota High School Activities Association to reverse its policy on allowing trans students to compete in the sports activities that align with their gender identity. And is far too often the case in America, where a few Republicans strongarm the majority into the corner, over 80% of school administrators who participated in a 2019 survey support the current, trans-inclusive policy.
Meanwhile, coming in from the Congressional side, Senator Kelly Loeffler of Georgia put forward a bill that would explicitly state that allowing trans girls and women to compete in women’s sports is a violation of Title IX. That’s repulsive enough but, in a further violation of trans women’s and girls rights, the bill even allows for schools to require students to undergo “genital exams” to prove they aren’t transgender. This is beyond horrifying. Earlier this year, a bill just like this passed in Idaho.
As if all this weren’t repulsive enough, the transparent hypocrisy and bigotry of all of this is glaringly obvious when, less than three weeks ago, Caster Semenya lost her case in the Switzerland supreme court. Semenya won’t be allowed to compete in women’s track and field (including upcoming Olympics, whenever those happen again) unless she medically reduces her natural testosterone levels. All of this — the verdict affecting Semenya, the anti-trans sports policies making their rounds — is about policing who gets to be a woman and what it means to be a woman, and it all fits hand in hand with the ongoing violations of reproductive rights that Rachel discusses below.
Earlier this week Xoài wrote an incredibly powerful call-in to TERFs like JK Rowling, making an irrefutable case that shouldn’t have needed to be made in the first place — that cis and trans women’s liberations are inextricably intertwined becuase we are, in fact, all women being repressed (in different ways, to different extents) by the same patriarchy. As anti-trans legislation continues to gain momentum around this country, we cis women must fight in solidarity.
Reproductive Rights
We Could Lose Roe v. Wade Next Year. What Now?
ICE Hysterectomy Doctor Wasn’t Even a Board-Certified OB-GYN
Rachel: The juxtaposition of these articles with each other seems like such an effective (and dark) way to highlight what we were talking about last week. As reproductive rights continue to be chipped away at, we’re seeing increasing efforts at exerting control over reproductive freedoms both in the form of restricting access to abortion and birth control and in reproductive violence like nonconsensual hysterectomies, police violence, zero or inadequate care for pregnant people, especially pregnant Black and indigenous women, and more. This is already happening, no doubt about it, and it is horrifying; the top article, however, does have some direct and concrete guidelines for action. They’re applicable not just to reproductive justice, but to what our communities will need in general now more than ever: look at who’s doing the work on the ground and locally, figure out what resources they need and help them access them; look at what individuals around you need to make it through and redistribute any resources you can toward them directly, rather than trusting big bureaucratic orgs or government agencies to provide for them.
They’re Being Empowered Even More and Becoming Emboldened
Florida Gov. Just Made It Easy for Drivers to Run Over Black Lives Matter Protesters
Himani: This one is beyond horrifying. Drivers can already get away with a lot in terms of severely injuring or even killing people with very, very little liability (if any). Now that’s been explicitly enshrined into Florida law by DeSantis.
A Notorious COVID Troll Actually Works for Dr. Fauci’s Agency
Neo-Nazi Terror Leader Said to Have Worked With U.S. Special Forces
“People’s Rights” Organizing Linked Directly to Ammon Bundy
Mysterious QAnon Conspiracy Theory Mailings Spook Minneapolis Suburbs
Rachel: I’m reading these stories about “people’s rights organizing,” QAnon mailings, and thinking about stories a few months back about the FBI’s fumbling attempt to start enacting Trump’s orders that “antifa” be treated as a terrorist group, namely this story. There’s the somewhat obvious parallel that the federal government is positioning antifa, which is… not even actually a group, as a terrorist group while glossing over what are quite literally and undeniably actual domestic terrorist groups. But I guess it feels like something more layered to me – maybe I’m thinking of how often the GOP mirrors the tactics of abusive and manipulative individual people in terms of how it accuses its opponents of not just things they aren’t doing, but the exact same things the GOP itself IS doing. (Think of the security accusations against Hillary while Trump was taking sensitive international calls on his personal cell phone, or the far-right handwringing over ‘freedom of speech’ while they remove historically accurate curriculum from schools for its honesty about chattel slavery and genocide.) I feel glumly like in the perpetual debate over whether the government is being intentionally evil or just stupid, this is a place where it feels increasingly like intentional malice, and I’m truly concerned about the propagation of what are unfortunately more and more like far-right terrorist cells, ones that are separate from but not uninvolved with the far-right police state – as an example, this chilling piece on just last night in Louisville, where riot police were filmed giving detailed instructions to armed MAGA militia on how to avoid their crowd control.
COVID-19 Update
When Nowhere Feels Safe: COVID-19, Anti-Asian Racism and Domestic Violence
Himani: Domestic violence has been a quietly accepted reality in many Asian American communities since long before the pandemic started. This in-depth feature takes a much-needed look at how the pandemic exacerbated an already-tenuous situation. I highly recommend this article.
Colleges’ Opening Fueled 3,000 COVID Cases a Day, Researchers Say
Himani: This is one of those times where I can’t help but say, “who’s surprised?” Reopening schools was an incredibly fraught decision, and I know that simply keeping schools and universities closed would also do irreparable harm to many, many communities. But the problem is that this country prioritized reopening the economy and trying to return life to normal at the expense of schools.
Pentagon used taxpayer money meant for masks and swabs to make jet engine parts and body armor
Harvard’s Chetty Finds Economic Carnage in Wealthiest ZIP Codes
Himani: This is yet another round of things everyone has already been saying for a long time but Raj Chetty comes in to verify the story and now, suddenly, it is irrefutable fact. I have nothing against Chetty, but it is somewhat infuriating how beholden to quantitative data and big analyses people are. This story isn’t new. It’s been reported on since the pandemic first started, and we’ve included just a fraction of those articles in this column. If more people in legislative offices are willing to take the issue seriously now that Chetty has weighed in, that’s ultimately a good thing. But I do wish we as a society thought about data and policy a little differently and stopped being so infatuated by the cult of genius.
And a Little Bit of Hope
The Left Is Remaking the World
Ilhan Omar Is Not Here to Put You at Ease
The Cop Who Quit Instead of Helping to Gentrify Atlanta
Rachel: This is extremely worthwhile reading, for a variety of reasons, but I want to emphasize especially the link here between police violence, gentrification, and Breonna Taylor’s murder — it’s not an exaggeration to say that a scheme exactly like this one is why Breonna was murdered in her home.
From this Mother Jones piece on gentrification in Atlanta:
On my beat, they started telling me: “We really want you to start policing this section of Boulevard and Ponce de Leon Avenue, basically the Bedford Pines Apartments. We think there are dope boys in there. We think there’s a lot of illegal activity happening and we want to really focus there. So we’re gonna put up signs that say you can’t park on the street. I want you to go and write tickets on every single car that’s on the street and I want you to get those cars out of there; if they don’t move, tow ’em. I want you to start running checks on everybody standing on the street; if they have got warrants, I want you to lock ’em up.”… “The only way you can evict or do anything like that is if the person who owns the apartment is convicted of a felony. So the Bedford Pines guys just went to the police department and said: “We want you to police in here, and we’re going to give you a section of Bedford Pines to actually have office space. And I want you to lock up as many people as possible so we can make these apartments vacant and we can knock ’em down.”
From this piece on the gentrification racket in Louisville:
Breonna Taylor’s shooting was the result of a Louisville police department operation to clear out a block in western Louisville that was part of a major gentrification makeover, according to attorneys representing the slain 26-year-old’s family. Lawyers for Taylor’s family allege in court documents filed in Jefferson Circuit Court Sunday that a police squad — named Place-Based Investigations — had “deliberately misled” narcotics detectives to target a home on Elliott Avenue, leading them to believe they were after some of the city’s largest violent crime and drug rings.
I know it can feel overwhelming and defeating to keep up with and even consider working against all the forms of violence and oppression we’re dealing with right now – it may or may not make it feel more manageable to remember that they aren’t actually different forms of violence and oppression; many of them are arms of the same tree, and remembering the end goal of felling the trunk (roots? This analogy got away from me a bit) is the way to keep focus and perseverance.
Newsom orders 2035 phaseout of gas-powered vehicles, calls for fracking ban
Historic settlement inches closer in South Dakota land dispute
Himani: One of the activists involved in making this happen, William Bear Shield, said, “I think whatever happened, happened in the past. I don’t know that there’s any changing that. All I know is that at some point, you can right a wrong.”
Those are words to live by, now more than ever.
Extra! Extra! will be moving to a biweekly schedule for the month of October, starting next week. We’ll see you in two weeks!
Raising Baby T. Rex: How Being a Mom Changed My Mind About Abortion
The protestors outside of the Planned Parenthood office I worked at eventually started heckling me by name. I knew their names, too, the regular ones, at least. The ones who owned the so-called crisis pregnancy center in the plaza next to our office. The ones who shrieked at us as we went into the office to do our jobs. The ones who hurled emotionally abusive insults at patients, pleading with them to save their babies, calling them murderers and sinners as the patients ignored their pleas. It was a regular part of my day when I worked for a Planned Parenthood affiliate in my early-to-mid twenties.
I started to take pride in the ways these zealots obviously followed me and my work in our community. They started tailoring the insults to be about my queerness, specifically. They’d yell that I was a dyke and that I was going to hell for being gay as well as for being a murderer. Mostly, it didn’t matter too much to me. We had a large parking lot. They couldn’t get physically close.
There were times when I got scared, though, like when I stayed late into the evening and was the last one out and had to walk to my car alone. Or this one time after dark when I saw a small, bright red light shining towards the building from inside a black SUV that was pulled up right outside the door. It turned out to be a light from a handheld device and the guy parked against the curb was picking up our medical sharps. Still, I had a momentary thought that it could be a sniper rifle just waiting for a worker to come into view.
I was just an entry-level community organizer. I can’t imagine how our abortion doctor and medical staff felt. Or our CEO. If you’ve never worked in an abortion provider’s office, you might not know that they usually have bulletproof glass around the reception desks or that the mail is all pre-opened by an administrator wearing latex gloves (in case there are harmful powders or sinister items in the envelopes). If you have worked in an abortion provider’s office, you know these things are routine and eventually become quite normalized.
Ironically, the first time I had anti-abortion hate mail delivered specifically to me was during my first week at my new job, in a small office of the ACLU of NY. We were a tiny staff of two. We didn’t have bulletproof glass or a secure entry or a process for opening suspicious mail. It was fine. It was just a hateful note and some literature. I was suddenly aware, though, of how much I took all those security measures for granted.
It’s still a dangerous time, even more dangerous, I might argue, for patients, medical providers, staff, and activists working in the repro health, rights, and repro justice fields. That hasn’t changed. It may even be worse.
I realized on the anniversary of Roe v. Wade this year that it’s the first year since 2005 that I haven’t been working for an org that is actively engaged in repro rights work. I will always align myself with the repro justice movement, even when I was working within more repro rights-based organizations. (There’s a difference between repro rights and repro justice.) I definitely see my current job at Bitch Media as aligned with repro justice. However, my role there isn’t directly engaged in advocacy and for the first time I am not a part of the organized movement in my professional or personal life. That’s a big shift for me.
The second reflection that came to me on the Roe anniversary was that I am even more committed to abortion access as a mom and as an adoptee. As an adoptee, I always felt a little tension between the narrative that adoption was the “ethical choice” pushed by evangelicals and extremists. I was afraid to speak ill of being adopted. Obviously, it worked out for me! But the reality is that pregnancy and giving birth is not an easy peasy thing. Separating a newborn baby from the person who carried them and shared blood with them for ten months is not as easy as filling out adoption paperwork. I didn’t know how to articulate it until I had my own, very planned, costly, mostly easy pregnancy and childbirth.
Now I know. There’s an emotional impact that’s innate to pregnancy at every stage. There are reactions you don’t know you’re going to have and, whether you want it or not, a very real physical tethering between you and the little fetus alien t-rex zapping your nutrients and energy. Even if you can ignore or don’t have any maternal or parental attachment to your pregnancy, pregnancy does stuff to your body that’s just goddamn hard. It affects your ability to work and keep employment, in some cases. It affects your relationships with other adult humans. It affects how people see you and react to you. It makes you feel out of control of your own body and I can only imagine that it’s much worse if you didn’t feel that you were able to make the deeply personal decision to be pregnant on your own terms.
I was proudly pro-abortion before I was a mom. I’ve doubled down on that belief after becoming one. What once seemed common sense to me — people should be able to make their own decisions about health care, pregnancy, and parenting — has become even more radical. It is inhumane to deny a person the agency to make their own informed, stigma-free decisions about abortion, adoption, birth control, and parenting. I believe that with my whole soul.
The sidewalk protestor in my head is saying, “What if your mom had aborted you?” That’s a real thing they’ve yelled at me, ya’ll. As an adoptee, it always stung in a particularly abandonment-triggering way. Now, honestly, my answer would be:
“If I could go back and give my parent or parents the freedom to have an abortion if they wanted one, I would wholeheartedly want that for them. I was abandoned, left completely alone when I was just one-year-old, and I’m extremely lucky that my life is as rich and safe and full of love as it is. Adoptees experience real harm from being given up for adoption, even at a young age. Gestational parents experience real harm from being made to give their children up, particularly if they were led to believe that was their only choice. Being happy for my life and deeply loving my family is not the same as believing that my gestational parent should have been made to carry me to term. If my ‘mom had aborted [me],’ that would have been her decision and I wouldn’t be here to have an opinion about it and that truly is a-OK with me.”
When I look at Remi, I feel such joy and I know what it means to make a parenting decision completely on your own terms. I also think, “Wow, I never want to be pregnant or raise a newborn again.” I can make that decision. To have that option is a huge privilege, one I will always fight for every person to have.
3 Queer Parenting Things I’m Currently Overprocessing
1. Things I Definitely Said Outloud This Month
- I said no food in the bathroom.
- No way. You can not hide those in my crotch.
- Head-to-back: You can only pet the cat in one direction.
- Do you need to go in time out… or are you going to put your shirt on?
2. Waffle’s Newest Snow Baby
Big surprise. Remi loves the snow! We’re officially past the age where we get excited about snow. We live in a four-season region of the Northeastern United States. Snow is pretty for a second and then you have to leave your house and it’s a lot less enjoyable.
As with anything, kids make snow more bearable because they love it so much. Every morning before school, Remi tries to get every last second of snow time before I make her get in our car.
http://www.instagram.com/p/B7JXoemhRqP/
She also “helps” us shovel the driveway and sidewalk and her new favorite thing is being buried under the snow (only when she has snow pants on). She even, somehow, got us to lie down in the snow, which is quite a thing because it is not 100% definite that either of us will be able to get back up.
3. Baby T.’s First Chopsticks!
For Christmas, Remi got a pair of training chopsticks (with a rice spoon!) and she’s so happy using them! Whenever I’d use chopsticks, she wanted in on the action, but she could only wield one at a time and her technique was primarily stabbing.
http://www.instagram.com/p/B6ya36HB_Fx/
I’m happy to be starting her early. I learned how to use chopsticks from the back of a paper wrapper in a Chinese restaurant. I just finally got my own Korean chopsticks (with rice spoons!) this Christmas. I’m trying to level up my Korean culture. Baby steps!